Navigating primary sclerosing cholangitis: Diagnosis and the 5 pillars of management
Primary sclerosing cholangitis remains a challenging disease to diagnose and manage, due to varying presentations, associated disease processes, and lack of targeted treatment.
-
02/01/2026
-
by Judy A. Trieu, MD, MPH , Mahesh Krishna, MD , David N. Assis, MD
Primary sclerosing cholangitis (PSC) remains a challenging disease to diagnose and manage, due to varying presentations, associated disease processes, and lack of targeted treatment.
In this issue’s In Focus, Drs. Mahesh Krishna and David N. Assis describe the diagnostic approach when PSC is suspected. Once diagnosed, they emphasize the five pillars of managing patients with PSC: malignancy, infection, fibrosis, symptoms, and inflammatory bowel disease activity.
Judy Trieu, MD, MPH, Editor in Chief
The New Gastroenterologist
What is primary sclerosing cholangitis?
Primary sclerosing cholangitis (PSC) is a chronic autoimmune liver disease characterized by inflammation and fibrosis of the intra- and extrahepatic bile ducts.1 A significant source of the morbidity and mortality in PSC consists of the elevated risk of malignancy, including cholangiocarcinoma, colorectal cancer, and gallbladder cancer.2 Disease progression in PSC is difficult to predict as there are no validated surrogate markers for clinical outcomes, such as cirrhosis, death, or cancer.
Patients with PSC often have elevated levels of alkaline phosphatase (ALP), a serum marker of cholestasis that is often used to assess clinical disease activity. However, ALP is limited by significant inter and intra-individual variation, and therefore may not consistently prognosticate disease progression.3 Emerging prospective data from the FICUS study by the International PSC Study Group evaluated transient elastography (TE) for liver stiffness measurement (LSM), to predict outcomes in PSC.4 First presented at EASL 2024, data showed that LSM by TE was strongly and independently correlated with overall survival and need for liver transplantation. Specifically, transplant-free survival at 5 years was 93.8% with LSM < 9.3 kPa, 79% with 9.6-14.3 kPa, and 48.1% with > 14.4 kPa, suggesting that LSM should be routinely incorporated into the clinical care and risk-stratification of patients with PSC.5
When should PSC be suspected?
The typical demographic of PSC was traditionally thought to be that of a young adult male. Indeed, most patients are male, an unusual demographic for an autoimmune disease. However, PSC can present at any age and in any sex, race, or ethnicity; and so it should be suspected in anyone with suggestive clinical signs or symptoms.6 About half of patients are asymptomatic at diagnosis, but the most common presenting symptoms within the first few years of diagnosis include fatigue, abdominal pain, pruritus, and depression.1
The diagnostic modality of choice in PSC is magnetic resonance cholangiopancreatography (MRCP) with the typical features including intra- and/or extra-hepatic strictures alternating with normal or dilated bile ducts, although a negative MRCP does not exclude PSC in the setting of high pretest probability.7 Due to the advancements in MRCP imaging quality and non-inferiority of MRCP for PSC diagnosis, ERCP is not recommended for diagnosis along with procedural risks of pancreatitis and biliary tract seeding.7
PSC should be suspected in any patient with elevation in cholestatic enzymes such as ALP or γ-glutamyltransferase, especially in a patient with pre-existing IBD. 4 PSC has a very strong association with inflammatory bowel diseases (IBD), detected in up to 80% of cases, while approximately 5% of patients with IBD have PSC.1 PSC-IBD has unique characteristics of intestinal inflammation including higher prevalence of extensive colitis, worsened right-sided colonic disease with backwash ileitis, and clinically mild disease. Colitis in PSC-IBD also significantly increases the risk of colorectal cancer compared to IBD alone.1,8 Therefore, PSC-IBD should be considered a unique clinical entity, and the standard manifestation of the disease.
Furthermore, in one cohort study that empirically screened all IBD patients with MRCP, up to 7.5% had biliary PSC-like strictures, even though many had no symptoms nor laboratory abnormalities9. However, preemptive MRCP screening of IBD patients, in the absence of abnormal cholestatic labs or symptoms, is not currently recommended. Interestingly, the rate of IBD in African American patients with PSC is lower (60%) compared to the general population (80%), so there should be a lower threshold to suspect PSC in this demographic with elevated cholestatic enzymes, even without intestinal inflammation.6
In patients without IBD, causes of secondary sclerosing cholangitis should be closely scrutinized and ruled out such as HIV, ischemia, malignancy, IgG4 disease, sarcoidosis, and immunotherapy related diseases.7 According to AASLD practice guidance, and EASL practice guidelines, all patients with suspected PSC should have serum IgG4 levels obtained once to rule out IgG4-sclerosing cholangitis.7,10
Small-duct PSC is denoted by histological findings of PSC on liver biopsy in the absence of biliary strictures on MRCP and clinical presentation is similar to large-duct PSC although small-duct PSC does not have the risk of acute biliary obstruction or cholangitis.7 Small-duct PSC carries a more favorable prognosis but can develop into large-duct PSC in up to a quarter of patients.7 Therefore, MRCP should be repeated every 3-5 years for these patients.7
How should PSC be managed?
There are currently no FDA-approved treatments for PSC. Historically, ursodeoxycholic acid (UDCA) was repurposed from PBC for patients with PSC. The initial randomized controlled trial of UDCA in PSC, published in the New England Journal of Medicine in 1997, showed that 13-15 mg/kg of UDCA improved ALP, total bilirubin, and aspartate aminotransferase at 1 and 2 years.11 However, there was no difference in overall transplant-free survival, nor has this been demonstrated in subsequent trials. One clinical trial using high-dose UDCA (28-30 mg/kg) reported an increased rate of adverse events, and this dosing should not be used.7,11
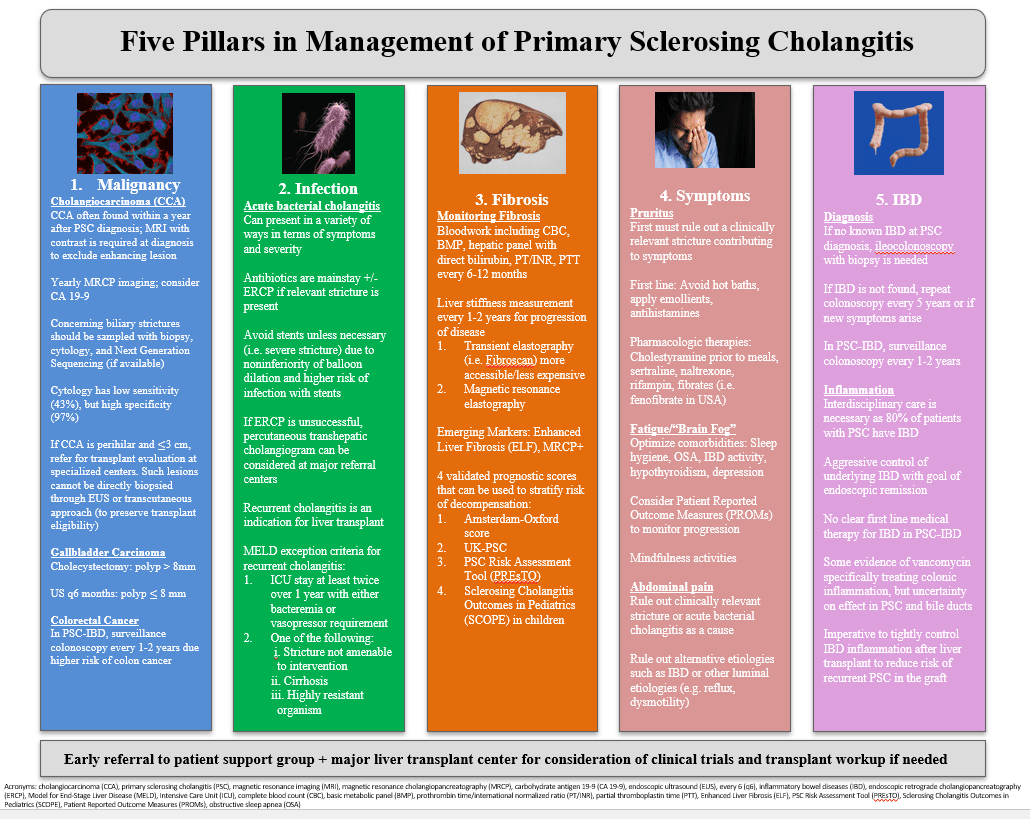
Due to the lack of effective therapy, all patients with PSC should be referred to specialized centers for consideration of enrollment in clinical trials. If a patient with elevated cholestatic serum tests is not eligible or interested in clinical trials, moderate UDCA doses (13-23 mg/kg/day) can be prescribed to reduce cholestatic markers, given that reduced cholestatic markers may impact long-term outcomes in some patients based on retrospective data.12,13 However, this should not substitute for the urgent need for innovative therapies in PSC, and many recent clinical trials allow patients treated with ongoing UDCA to enroll. There are five pillars (Figure 1) that every clinician should be mindful of when managing patients with PSC: malignancy, infection, fibrosis, symptoms, and IBD activity.
Malignancy. The first major pillar of PSC management includes screening for malignancy due to a significantly higher risk compared to the average population. Cholangiocarcinoma is the most feared complication of PSC with the highest risk within the first year of diagnosis and up to a 20% risk of the cancer at 30 years after diagnosis.7 Guidance from the AASLD recommends MRCP with or without carbohydrate antigen 19-9 (CA 19-9) yearly to monitor for the development of cholangiocarcinoma. CA 19-9 is neither fully specific or sensitive for cholangiocarcinoma and often will be elevated at baseline in patients due to cholestasis. However, when combined with MRCP, a CA 19-9 cutoff of 20 U/mL may increase the sensitivity up to 100%, while a cutoff of 129 U/mL may actually have a specificity up to 98%.7 In contrast, EASL guidelines recommend against checking a CA 19-9 due to it limited accuracy, though yearly imaging with MRCP is recommended.10 In patients with cirrhosis, more frequent imaging to monitor for hepatobiliary malignancy, including hepatocellular carcinoma, is recommended every 6 months.10
Patients with PSC also have an elevated risk of gallbladder carcinoma (9-78 times greater than the general population) and attention should be given to the gallbladder on yearly imaging.7 Patients with a gallbladder polyp >8 mm should be immediately referred for an evaluation for cholecystectomy while those with a polyp ≤8 mm should have surveillance ultrasound imaging every 6 months.7
Patients with PSC-IBD also have an increased risk of colorectal cancer compared to the general population and compared to patients with IBD alone. Colonoscopy with segmental biopsies should be performed at diagnosis of PSC to rule out concomitant IBD, if not already diagnosed.
Infection. The second major pillar in managing PSC is the treatment of infections such as bacterial cholangitis, a common complication of the disease due to biliary strictures and bacterial colonization of the biliary tree. Bacterial cholangitis can present in a variety of ways and there is currently no consensus definition for a true episode of bacterial cholangitis in PSC. The presentation of acute cholangitis typically includes abdominal pain, fevers, and jaundice; however not all patients present with classic findings of the Charcot’s Triad and thus the threshold to suspect cholangitis in PSC should be low.
Some patients present with sepsis and bacteremia. Others present with less severe fevers and elevated cholestatic markers, while the mildest cases display only minor symptoms that are relieved with antibiotics.10 Oral amoxicillin/clavulanic acid is often administered for milder cases, while piperacillin/tazobactam or a third generation cephalosporin with anaerobic coverage is used in cases of bacteremia requiring intravenous antibiotics.10 Temporary biliary stents are often necessary for management of severe strictures, though for milder strictures, they should be avoided due to their non-inferiority to balloon dilation but increased risk of bacterial cholangitis.14
Fibrosis. The third pillar is monitoring for signs of liver fibrosis progression to cirrhosis. Patients with PSC should receive bloodwork every 6-12 months monitoring liver enzymes including aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, total and direct bilirubin, albumin level, γ-glutamyltransferase as well as a complete blood count (monitoring platelets closely) and basic metabolic panel (monitoring sodium and creatinine), as well as a coagulation panel. Per EASL guidelines, LSM, either by TE or magnetic resonance elastography, should be performed every 2-3 years to monitor for progression of disease.10
Based on emerging data, it is reasonable to monitor with a LSM yearly, due to its validated prognostic value6. Another emerging option, not yet widely available, is serum fibrosis testing with the Enhanced Liver Fibrosis (ELF) score, comprising of serum markers associated with fibrosis development such as hyaluronic acid, tissue inhibitor of metalloproteinase-1, and procollagen type III N-propeptide. Currently, there is an effort by the International PSC Study Group, funded by PSC Partners Seeking a Cure, to validate ELF as a prognostic marker of clinical outcomes, similar to the FICUS study with TE. One other option to monitor risk of hepatic decompensation or liver transplantation is to utilize a validated clinical prognostic model for PSC such the Amsterdam-Oxford score, UK-PSC, and PSC Risk Assessment Tool (PREsTO) for adults and Sclerosing Cholangitis Outcomes in Pediatrics (SCOPE) for children.7 However, these tools should be used with caution in individual patients until further validation. Patients with cirrhosis should be referred to a transplant center with experience in PSC.
Symptoms. Addressing symptoms such as pruritus, fatigue, “brain fog”, and abdominal pain comprise the fourth pillar of PSC management. Pruritus can occur with or without biliary strictures, but new onset of itch should prompt laboratory studies and an MRCP for evaluation of a culprit clinically-relevant stricture. First line management should include counseling on avoiding heat and hot baths, utilizing topical emollients, and antihistamines such as hydroxyzine. If these are ineffective, therapy with a bile acid sequestrant, such as cholestyramine (4-16 mg), can be attempted, though it is associated with gastrointestinal side effects.7 Other options for pruritus not responsive to initial management include sertraline, naltrexone, and rifampin.7 Importantly, the FITCH trial recently demonstrated that fibrates, such as fenofibrate and bezafibrate (not available in the U.S.), are effective at reducing cholestatic itch in patients with PBC and PSC15 and this option should also be considered. Lastly, ileal bile acid transporter inhibitors (IBAT-i) are an emerging therapy for management of cholestatic pruritus in PBC and PSC.16
Fatigue and “brain fog” are much more difficult symptoms to manage with optimization of other potential underlying causes such as sleep hygiene, obstructive sleep apnea, and hypothyroidism as good initial steps. Other techniques such as mindfulness have previously been shown to improve symptoms in patients with autoimmune hepatitis and similar programs are under active investigation in PSC.17
Right upper abdominal pain is also a frequent symptom in patients with PSC, and the first step of management is to rule out worsening biliary obstruction or acute cholangitis. However, other causes such as underlying IBD or upper gastrointestinal disorders should also be considered. The best way to objectively measure symptoms that can be utilized in a clinical trial is through a patient reported outcome measure (PROM). The Simple Cholestatic Complaints Score is a validated PROM in the Netherlands that utilizes pruritus, fatigue, right upper quadrant abdominal pain, and fever.18 This score is currently under investigation for validation in other countries such as the United States. Additionally, patient-driven PROMs for individual symptoms are currently being developed by PSC Partners Seeking a Cure. Given the fluctuating nature of alkaline phosphatase in PSC, PROMs are a potential solution in obtaining FDA-approval for a drug that improves patient’s overall quality of life.
Inflammatory Bowel Disease. The fifth pillar of management of PSC is control of underlying IBD. Often, care for PSC is provided by a transplant hepatologist and the IBD component will be managed separately by a general gastroenterologist or IBD specialist. However, these dual disease manifestations are integrally related, and interdisciplinary care is crucial due to the potential of these diseases to interact with each other. Recent work from the International PSC Registry found that colectomy was associated with decreased risk of liver transplantation or death with the most pronounced effect in patients with proctocolectomy with permanent ileostomy.19 Additionally, active IBD post-liver transplant can increase the rate of graft failure, is an independent risk factor for recurrent PSC, and can lead to worse outcomes.20 There is not enough evidence to strongly recommend one biologic over another in PSC-IBD. Interestingly, although vedolizumab acts mechanistically on the gut-homing pathophysiology in PSC and is well-suited to treat IBD in PSC patients, it has not been found to benefit liver inflammation.21 Close monitoring of disease activity and tight control of colonic inflammation is essential.
Emerging therapies for PSC
There are currently no approved therapies for PSC, however new options are emerging. One molecule under investigation is 24-norurosdeoxycholic acid (norucholic acid), a shortened version of UDCA with one less methyl group, preventing conjugation by taurine or glycine, which allows increased cholehepatic shunting and increased anti-inflammatory and anti-fibrotic effects.22 Recently, Phase 3 clinical trial results (n=301) for norucholic acid (NCT03872921) achieved the primary endpoint of partial normalization of alkaline phosphatase without worsening of fibrosis by liver biopsy (15.1% versus 4.8%).23 Furthermore, 25% of participants in the treatment group, versus 10% in the control, improved by 1 stage of fibrosis on follow-up liver biopsy at 96 weeks. 23 Other drugs under investigation fall into major themes including modulating the immune system, gut microbiome (such as with vancomycin and bacteriophages), bile acid circulation (PPAR agonists, IBAT inhibitors), and fibroblast response (anti-fibrotics such as CM-101).4,24
Conclusion
PSC is an autoimmune liver disease that can lead to cirrhosis, recurrent cholangitis, or cholangiocarcinoma and currently has no available disease-modifying treatments. All patients with PSC should be referred to specialized centers where they can be considered for enrollment into clinical trials. There are five pillars that should be considered in PSC disease management: malignancy, infection, fibrosis, symptoms, and inflammatory bowel disease. New therapies are under active investigation for PSC with norucholic acid the closest to approval in Europe. PSC is one of the greatest unmet needs in gastroenterology and hepatology that will need much more work done in the years ahead to improve patient care and outcomes.
Conflicts of Interest: Dr. Krishna has consulted for Ipsen but does not have an active relationship. Dr. Assis has no relevant disclosures.
References
Manns MP, Bergquist A, Karlsen TH, et al. Primary sclerosing cholangitis. Nat Rev Dis Primers. Mar 13 2025;11(1):17. doi:10.1038/s41572-025-00600-x
Boonstra K, Weersma RK, van Erpecum KJ, et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology. Dec 2013;58(6):2045-55. doi:10.1002/hep.26565
Trivedi PJ, Muir AJ, Levy C, et al. Inter- and Intra-individual Variation, and Limited Prognostic Utility, of Serum Alkaline Phosphatase in a Trial of Patients With Primary Sclerosing Cholangitis. Clin Gastroenterol Hepatol. Jun 2021;19(6):1248-1257. doi:10.1016/j.cgh.2020.07.032
Assis DN, Bowlus CL. Recent Advances in the Management of Primary Sclerosing Cholangitis. Clin Gastroenterol Hepatol. Jul 2023;21(8):2065-2075. doi:10.1016/j.cgh.2023.04.004
Chazouillères O, Schramm C, Trivedi PJ, et al. GS-007 Prospective validation of the prognostic value of liver stiffness assessed by Fibroscan in primary sclerosing cholangitis: final results of the FICUS study. Journal of Hepatology. 2025/10/14 2024;80:S5.
Goldberg DS, Levy C, Yimam K, et al. Primary Sclerosing Cholangitis Is Not Rare Among Blacks in a Multicenter North American Consortium. Clin Gastroenterol Hepatol. Apr 2018;16(4):591-593. doi:10.1016/j.cgh.2017.10.028
Bowlus CL, Arrivé L, Bergquist A, et al. AASLD practice guidance on primary sclerosing cholangitis and cholangiocarcinoma. Hepatology. Feb 01 2023;77(2):659-702. doi:10.1002/hep.32771
Trivedi PJ, Crothers H, Mytton J, et al. Effects of Primary Sclerosing Cholangitis on Risks of Cancer and Death in People With Inflammatory Bowel Disease, Based on Sex, Race, and Age. Gastroenterology. Sep 2020;159(3):915-928. doi:10.1053/j.gastro.2020.05.049
Lunder AK, Hov JR, Borthne A, et al. Prevalence of Sclerosing Cholangitis Detected by Magnetic Resonance Cholangiography in Patients With Long-term Inflammatory Bowel Disease. Gastroenterology. Oct 2016;151(4):660-669.e4. doi:10.1053/j.gastro.2016.06.021
Liver EAftSot. EASL Clinical Practice Guidelines on sclerosing cholangitis. J Hepatol. Sep 2022;77(3):761-806. doi:10.1016/j.jhep.2022.05.011
Lindor KD. Ursodiol for primary sclerosing cholangitis. Mayo Primary Sclerosing Cholangitis-Ursodeoxycholic Acid Study Group. N Engl J Med. Mar 06 1997;336(10):691-5. doi:10.1056/NEJM199703063361003
Al Mamari S, Djordjevic J, Halliday JS, Chapman RW. Improvement of serum alkaline phosphatase to <1.5 upper limit of normal predicts better outcome and reduced risk of cholangiocarcinoma in primary sclerosing cholangitis. J Hepatol. Feb 2013;58(2):329-34. doi:10.1016/j.jhep.2012.10.013
Hilscher M, Enders FB, Carey EJ, Lindor KD, Tabibian JH. Alkaline phosphatase normalization is a biomarker of improved survival in primary sclerosing cholangitis. Ann Hepatol. 2016;15(2):246-53. doi:10.5604/16652681.1193721
Ponsioen CY, Arnelo U, Bergquist A, et al. No Superiority of Stents vs Balloon Dilatation for Dominant Strictures in Patients With Primary Sclerosing Cholangitis. Gastroenterology. Sep 2018;155(3):752-759.e5. doi:10.1053/j.gastro.2018.05.034
de Vries E, Bolier R, Goet J, et al. Fibrates for Itch (FITCH) in Fibrosing Cholangiopathies: A Double-Blind, Randomized, Placebo-Controlled Trial. Gastroenterology. Feb 2021;160(3):734-743.e6. doi:10.1053/j.gastro.2020.10.001
Trauner M, Karpen SJ, Dawson PA. Benefits and challenges to therapeutic targeting of bile acid circulation in cholestatic liver disease. Hepatology. Oct 01 2025;82(4):855-876. doi:10.1097/HEP.0000000000001438
Alrabadi LS, Dutton A, Rabiee A, et al. Mindfulness-based stress reduction may decrease stress, disease activity, and inflammatory cytokine levels in patients with autoimmune hepatitis. JHEP Rep. May 2022;4(5):100450. doi:10.1016/j.jhepr.2022.100450
van Munster KN, Dijkgraaf MGW, van Gennep S, Beuers U, Ponsioen CY. The Simple Cholestatic Complaints Score is a valid and quick patient-reported outcome measure in primary sclerosing cholangitis. Liver Int. Nov 2020;40(11):2758-2766. doi:10.1111/liv.14644
Mol B, van Nieuwamerongen M, Färkkilä M, et al. DOP14 Proctocolectomy is associated with improved transplant-free survival in patients with primary sclerosing cholangitis: results from a pooled collaborative international study. 10/15/2025 2024;18(Supplement_1):i97-i98.
van Munster KN, Bergquist A, Ponsioen CY. Inflammatory bowel disease and primary sclerosing cholangitis: One disease or two? J Hepatol. Jan 2024;80(1):155-168. doi:10.1016/j.jhep.2023.09.031
Shah A, Jones MP, Callaghan G, et al. Efficacy and safety of biologics in primary sclerosing cholangitis with inflammatory bowel disease: A systematic review and meta-analysis. Hepatol Commun. Jan 01 2024;8(1)doi:10.1097/HC9.0000000000000347
Fickert P, Hirschfield GM, Denk G, et al. norUrsodeoxycholic acid improves cholestasis in primary sclerosing cholangitis. J Hepatol. Sep 2017;67(3):549-558. doi:10.1016/j.jhep.2017.05.009
Trauner M, Trivedi P, Denk G, et al. Norucholic acid for the treatment of primary sclerosing cholangitis: 96-week analysis of a pivotal phase 3 trial. 2025.