A newly updated AGA clinical care pathway outlines a streamlined, stepwise approach to screening, risk stratification, and treatment of metabolic dysfunction–associated steatotic liver disease (MASLD), emphasizing broader screening of high-risk patients and integrating newly approved pharmacologic therapies.
MASLD — formerly known as nonalcoholic fatty liver disease — affects about 30% of US adults and up to 65% of people with type 2 diabetes, making it one of the most common liver conditions seen in clinical practice. The updated pathway, published in Gastroenterology and developed by a multidisciplinary panel convened by AGA, reflects new disease nomenclature, advances in noninvasive testing, and the emergence of FDA-approved therapies for metabolic dysfunction–associated steatohepatitis (MASH).
The pathway is designed for use across multiple specialties, including primary care, endocrinology, cardiology, and gastroenterology/hepatology, where most patients with MASLD are evaluated and managed.
Expanded screening for high-risk groups
A revision of the 2021 version, the pathway prioritizes identifying patients at risk for clinically significant liver fibrosis, defined as stage F2 or higher, which is the strongest predictor of liver-related outcomes.
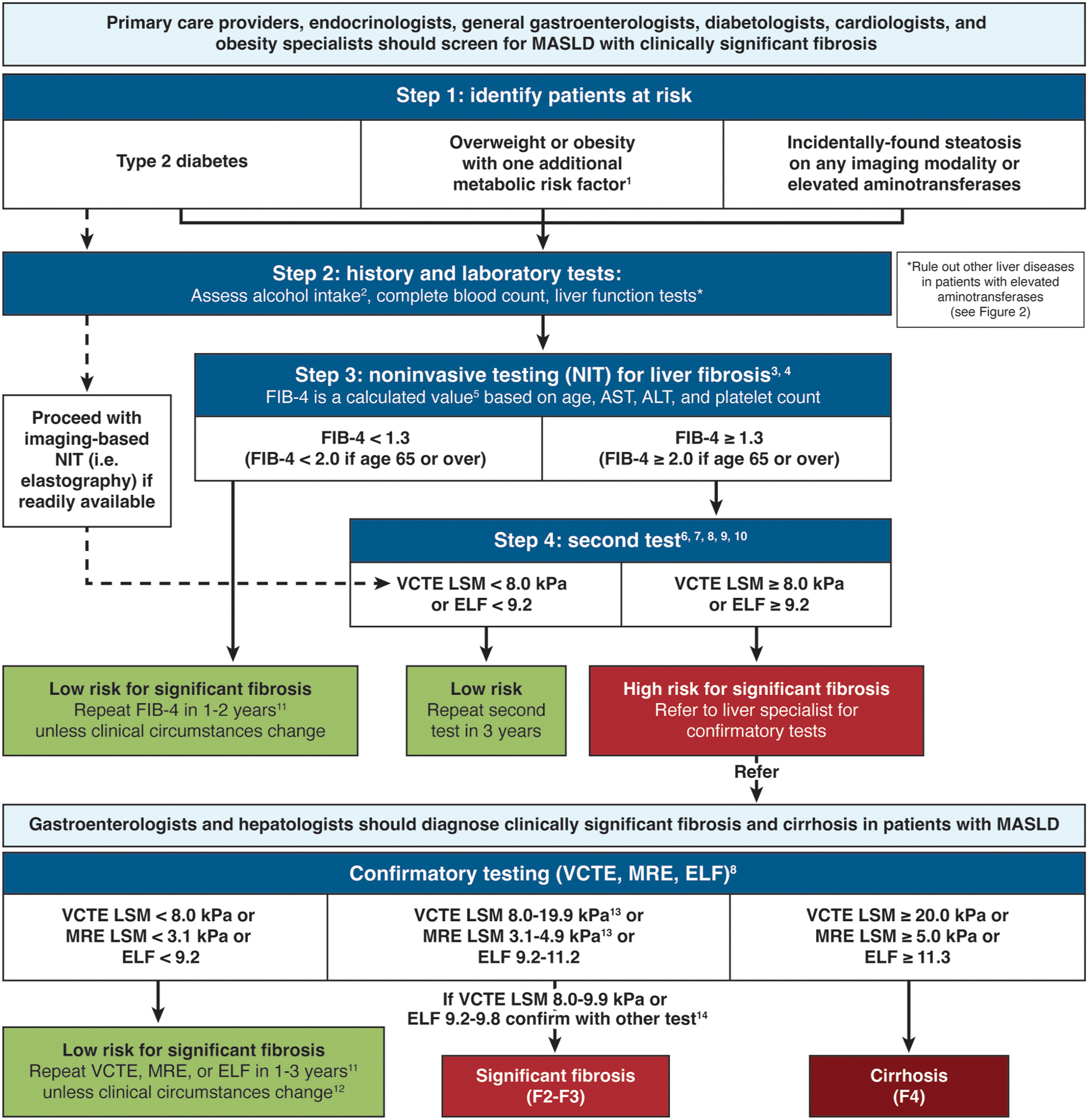
Clinicians are advised to screen three main groups:
Patients with type 2 diabetes
Individuals with overweight or obesity plus at least one additional metabolic risk factor
Patients with incidental hepatic steatosis on imaging or elevated aminotransferase levels
Clinically significant fibrosis occurs in about 14% of overweight or obese individuals and up to 20% of those with MASLD. Among patients with type 2 diabetes and MASLD, roughly 35.5% have advanced fibrosis (F2–F4), according to evidence reviewed by the task force, led by first author Fasiha Kanwal, MD, MSHS, of the Section of Gastroenterology and Hepatology in the Department of Medicine at Baylor College of Medicine, Houston
Because abdominal ultrasound has limited sensitivity for mild steatosis, the pathway suggests clinicians may proceed directly to fibrosis risk stratification in high-risk populations rather than relying on ultrasound for initial diagnosis.
Two-step risk stratification
A two-tier strategy is recommended using noninvasive tests to identify patients who require specialty evaluation.
The first step uses the fibrosis-4 (FIB-4) index, calculated from routine laboratory values. A FIB-4 score below 1.3 (or below 2 for patients aged 65 years or older) reliably excludes advanced fibrosis, with negative predictive values of 90% or higher. Patients with low scores can remain in primary care with repeat testing every one to two years. Those with FIB-4 scores at or above these thresholds should undergo second-tier testing.
The second step involves imaging-based liver stiffness measurement, typically vibration-controlled transient elastography. A liver stiffness value below 8 kilopascals indicates low risk for clinically significant fibrosis, whereas values of 8 kPa or higher should prompt referral to hepatology for further evaluation.
When elastography is unavailable, the enhanced liver fibrosis blood test may serve as an alternative, with a cutoff of 9.2 used to detect clinically significant fibrosis.
Metabolic disease management
Aggressive management of cardiometabolic risk factors for all patients with MASLD, regardless of fibrosis stage, is recommended.
Lifestyle interventions — including weight loss, physical activity, and dietary changes — remain the foundation of treatment. Weight reduction of at least 5% can improve steatosis, while losses of 10% or more are typically required for histologic improvement in liver fibrosis. Pharmacologic therapy is tailored to disease severity and comorbid conditions.
For patients with MASLD at low risk of fibrosis, medications primarily target metabolic disease. This includes GLP-1 receptor agonists such as semaglutide or dual incretin therapies such as tirzepatide for weight loss and glycemic control.
For patients with clinically significant fibrosis, the pathway incorporates newer disease-specific treatments. Resmetirom, a thyroid hormone receptor-β agonist approved for MASH with F2–F3 fibrosis, improved both resolution and fibrosis in the phase 3 MAESTRO-NASH trial, with resolution rates of about 26%–30% compared with 9.7% in the placebo group.
Semaglutide has also demonstrated benefits in the phase 3 ESSENCE trial, achieving MASH resolution without worsening fibrosis in 63% of treated patients versus 34% of those receiving placebo.
Implementation challenges remain
Despite growing evidence and new therapies, the authors noted that real-world adoption of MASLD care pathways remains inconsistent. Barriers they cited include limited awareness among primary care clinicians, competing clinical priorities, and variability in access to noninvasive testing.
To address these challenges, the updated pathway includes a pragmatic implementation framework designed to help health systems integrate screening and management algorithms into routine workflows.
“The standardized, evidence-based Pathway can allow clinicians to care for a rapidly growing population of patients, most of whom are managed in primary care or endocrine clinics,” the authors wrote.
Clinical implications
For practicing gastroenterologists and hepatologists, the updated pathway provides a practical roadmap for identifying patients who require specialist care while enabling primary care clinicians to manage low-risk disease.
The key takeaway is the importance of systematic screening and staged evaluation using widely available noninvasive tests. Early identification of fibrosis allows clinicians to initiate targeted therapy and surveillance before complications such as cirrhosis or hepatocellular carcinoma develop.
With MASLD prevalence rising and new treatments entering clinical practice, the pathway aims to standardize care across specialties and improve outcomes for a growing population of patients with metabolic liver disease, noted the authors.
Dr. Kanwal is an investigator at the Institute for Clinical and Translational Research and the Veterans Administration Center for Innovations in Quality, Effectiveness, and Safety at the Michael E. DeBakey VA Medical Center, Houston. She is supported in part by the National Cancer Institute and the Cancer Prevention & Research Institute of Texas. Disclosures for the other study authors are available in the published article.
Expert insight
GI & Hepatology News invited Brian DeBosch MD, PhD, AGAF, Professor and Co-Division Chief of Gastroenterology, Hepatology & Nutrition at Indiana University School of Medicine, to weigh in on the care pathway.
In your opinion, what are the top clinical takeaways from this clinical care pathway?

Dr. DeBosch: Important changes in whom to screen, how to screen, and how to treat are included in this new pathway. The overall goal is to clarify which patients warrant screening, condense screening steps where it makes sense, and incorporate new, field-changing RCT data and FDA-approved therapies in the care pathway. This is a more complete and data-driven pathway than its first iteration.
The new pathway expands and at the same time limits whom to screen. Specifically, the new pathway indicates that patients with overweight or obesity should be screened with at least one cardiometabolic risk factor. However, patients with isolated overweight or obesity should not be routinely assessed based on recently published data.
The new pathway streamlined how to screen. For example, the simplified screening cutoffs using the Fibrosis-4 (FIB-4) score is simplified to 1.3 for patients under 65, whereas patients who previously would have been labeled with an “indeterminant" FIB-4 value (1.3-2.67) range can now be functionally considered to have a positive screen. Similarly, new data confirm the value < 8.0 kPa as an appropriately sensitive cutoff to demarcate low- and high-risk fibrosis in patients. Finally, the option is afforded to skip two-tiered screening in some high-risk (e.g. T2DM or patients evaluated in a referral center) in favor of single-step FibroScan screening and diagnosis. Very user friendly, overall.
Perhaps the most notable addition is the incorporation of new, gold-standard RCT data for novel FDA-approved MASH therapy that were reported in the interval since the original pathway. Prior therapies were limited by a paucity of evidence for efficacy, lack of significant weight-directed control. Now, resmetirom and semaglutide demonstrate efficacy in reversing hepatic fibrosis and inflammation, whereas semaglutide and tirzepatide demonstrate robust weight loss and insulin sensitization.
How might this care pathway affect patient care?
Dr. DeBosch: The new pathway streamlines and simplifies screening pathways and are quite directive in treatment recommendations. This makes diagnosing and treating MASH in the primary care setting more accessible, which might expand the overall population accessing care for this common and morbid disease.
What knowledge gaps remain, and what research should be done next?
Dr. DeBosch: There are at least three important gaps to address, ideally in the next pathway. First, how should we treat so-called “lean” MASH (MASH + BMI < 25)? Current agents are aimed at reducing intrahepatic fat and/or peripheral adiposity. However, it is possible that lean MASH is more immunologically driven, making the choice of best first-line agent less straight-forward. Second, there are no agents with published, large RCT data demonstrating reversal of F4 compensated cirrhosis. Thus, utility of deploying currently available agents in that population is not clear. Third, the degree to which the pathway applies equally to all settings exposes the larger issue, that we remain all too distant from the era of true precision medicine. The authors rightfully and admirably acknowledge disparities in MASLD/MASH in Hispanic populations, and worsened outcomes in Black patients. However, sufficient evidence is lacking on if and - if so, how - to deploy or modify the pathway for patients of distinct ethnicity or, more specifically, distinct genotypes.
Is there anything else you’d like to say about this clinical care pathway?
Dr. DeBosch: Overall this is a well-considered, evidence-based updated pathway that makes screening, treatment and implementation of the pathway feasible and useful in a broad range of settings from primary care to the tertiary academic medical center. Further evidence will be required regarding how to treat lean MASH populations, and how precisely to best use this pathway against highly advanced disease, or disease occurring across distinct genetic backgrounds.
Dr. DeBosch reported having no relevant disclosures.