Eating disorders are common, deadly, and underdiagnosed
Eating disorders (ED) are life-threatening, complex psychiatric conditions impacting patients along the entire biopsychosocial spectrum. EDs are characterized by persistent disturbances in eating behaviors, distressing thoughts and beliefs regarding food, weight, and body shape, and disruption of psychosocial functioning around food and eating.¹˒² These disorders include, but are not limited to, anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), and avoidant/restrictive food intake disorder (ARFID). Despite a lifetime prevalence of 2% to 5%, more than half of individuals meeting ED criteria go undiagnosed.³˒⁴
Basics relevant to GI practice
EDs are diagnosed using Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM-5-TR) criteria. While these criteria emphasize emotional and behavioral issues related to maladaptive eating, gastrointestinal (GI) symptoms are common and often the reason patients present for care.
Anorexia nervosa
AN is characterized by restriction of energy intake leading to significantly low body weight, intense fear of weight gain or becoming fat, and a disturbance in body image.² AN can occur in individuals of any body size and may be missed when clinicians rely on weight alone. Behavioral clues include rigid food rules, anxiety about dietary recommendations when advised to liberalize intake, calorie tracking, avoidance of dietary fats or carbohydrates, excessive exercise, and resistance to nutrition support. In GI settings, patients may present with reflux, delayed gastric emptying, early satiety, bloating, abdominal pain, or constipation related to malnutrition and slowed motility.⁵˒⁶
Bulimia nervosa
BN is characterized by recurrent binge eating and compensatory behaviors — such as self-induced vomiting, laxative misuse, and excessive exercise — to prevent weight gain.² Behavioral signs may include repeated requests for GI evaluation of symptoms temporally related to purging behaviors. Because patients often have weights within or above normative ranges, the diagnosis can be overlooked unless clinicians inquire directly and nonjudgmentally about binge–purge behaviors. In GI practices, patients may present with reflux refractory to treatment, dysphagia, dental enamel erosion, parotid gland enlargement, chronic sore throat, abdominal pain, bloating, diarrhea related to laxative misuse, or electrolyte abnormalities such as hypokalemia.⁷
Binge eating disorder

BED is characterized by recurrent binge-eating episodes without the compensatory behaviors seen in BN.² BED is strongly associated with weight stigma and internalized weight bias, both of which contribute to delayed care and increased psychological distress.⁸ Clues for BED include chronic dieting, restriction earlier in the day followed by evening overeating, and weight cycling. Physical cues can include metabolic abnormalities or poorly controlled GI symptoms despite multiple dietary eliminations. In GI settings, patients may present with reflux, bloating, postprandial abdominal pain, diarrhea, or exacerbations of disorders of gut–brain interaction (DGBI) following binge episodes. Importantly, recommending restrictive diets without screening may unintentionally perpetuate the binge–restrict cycle.
Avoidant/restrictive food intake disorder
ARFID is characterized by inadequate nutritional intake and weight loss, nutritional deficiencies, and/or reliance on nutritional supplements that is not driven by body image concerns but by sensory sensitivity, fear of aversive consequences (e.g., choking or vomiting), or low appetite.² Individuals often exhibit extensive food elimination beyond evidence-based recommendations. Physical findings may include micronutrient deficiencies, unintended weight loss, fatigue, and persistent GI complaints.
ARFID is increasingly recognized among individuals with DGBI, particularly irritable bowel syndrome (IBS), functional dyspepsia, and emetophobia. ⁹˒¹⁰
Why education is important as a GI physician
If you treat patients with GI disorders, you are likely treating patients with EDs. In one study, 98% of individuals with EDs met criteria for a DGBI, most commonly IBS.⁵ Given the underdiagnosis of EDs and the prevalence of GI symptoms in patients with EDs, many patients present to GI clinics without a known ED diagnosis.¹¹˒¹² Shared features such as dietary restriction, fear of food-related symptoms, weight fluctuations, bloating, and altered bowel patterns create substantial risk for missed or delayed recognition.
Why gastroenterologists may struggle to care for patients with EDs
EDs and GI symptoms frequently coexist. Yet despite this clinical overlap, many gastroenterologists feel underprepared to identify and manage EDs in practice. Several structural and educational blind spots contribute to this gap.
Implicit biases and difficulty identifying eating disorders in practice

Weight bias — explicit and implicit — impairs identification of EDs, especially in patients with normal or higher weights. Weight loss may be praised rather than explored. The rise of glucagon-like-peptide-1 (GLP-1) receptor agonists add complexity as these agents commonly cause nausea, vomiting, early satiety, bloating, and constipation — symptoms that overlap with DGBI and ED presentations. Symptoms may be attributed solely to medication effects without considering underlying disordered eating. Additionally, GLP-1 medications may be misused for weight control outside of clear medical indications. Without routine screening, EDs often remain invisible.
Limited education on overlap
Medical training on EDs is limited and often emphasizes rare, catastrophic GI complications (e.g., superior mesenteric artery syndrome, Boerhaave syndrome, or necrotizing sialometaplasia) rather than common chronic manifestations.
The amplified gut–brain axis
DGBIs are inherently bidirectional. The dysregulation of the gut-brain axis is intensified in EDs: restriction or purging worsen GI symptoms and GI symptoms further restrict intake, threatening recovery. GI providers are uniquely positioned to interrupt this reinforcing cycle of physiologic symptoms and maladaptive behaviors.
Elimination diets without screening
Elimination diets are widely used in celiac disease, IBS, eosinophilic esophagitis, and other GI disease states. Patients also self-impose restrictions to improve symptoms or due to an ED. Diets such as the low-FODMAP are often recommended without dietitian support, defined duration, or ED screening. Restrictive diets may reinforce food fears, increase rigidity, and worsen nutritional compromise. Recognizing these, AGA recommends screening for EDs and disordered eating prior to initiating the elimination phase of the low FODMAP diet.¹³ Similar caution should be used with any restrictive diet.
The role of the GI provider in managing symptoms
While many GI symptoms improve with nutritional restoration, not all resolve. Persistent symptoms can undermine recovery and warrant targeted treatment. GI care often involves adapting treatment paradigms for conditions such as functional dyspepsia, IBS, and constipation, with ED-specific considerations.
Bloating and distention
Bloating and distention may exacerbate body image distress. Binging may lead to aerophagia which can contribute to gaseous distention. In addition, constipation is a common trigger for bloating and distention and should evaluated for and treated early on (see below).¹⁴ Restrictive diets (e.g., low-FODMAP diet) should be avoided or used cautiously in collaboration with a registered dietitian. Digestive enzymes (e.g., lactase, FODZYME) may support dietary liberalization. Evaluation for small intestinal bacterial overgrowth (SIBO) and abdomino-phrenic dyssynergia (APD) may also be appropriate.
Constipation
Laxative use for constipation requires transparent discussion of prior purging behaviors. The most common form of outlet dysfunction constipation, dyssynergic defecation, may be more likely to persist after ED recovery, sometimes requiring pelvic floor physical therapy.¹⁵ Rectal exams, motility testing, and pelvic floor physical therapy should be conducted in a trauma-informed manner, as individuals with EDs have higher rates of prior sexual trauma.¹⁶
Abdominal pain
Neuromodulators (e.g., amitriptyline and duloxetine) may be effective, but caution is warranted due to potential polypharmacy in patients receiving other psychiatric treatments. Brain-gut behavioral therapies (e.g., hypnosis and cognitive behavioral therapy) are effective in-person or via digital app-based versions.
Screening and referral
Despite the significant overlap of ED and GI disorders, GI providers lack standardized screening tools, confidence in initiating conversations about eating behaviors, and clear referral pathways. A large retrospective cohort study demonstrated that nearly three-quarters of patients with EDs had been seen by GI providers, yet almost half were not in active recovery at the time of consultation; these represent missed opportunities for early identification and intervention.¹⁷
Validated screening tools specific to GI populations are limited. However, clinicians can incorporate targeted questions to distinguish restriction due to body image versus that driven by fear of GI pain (see table 1 for examples).

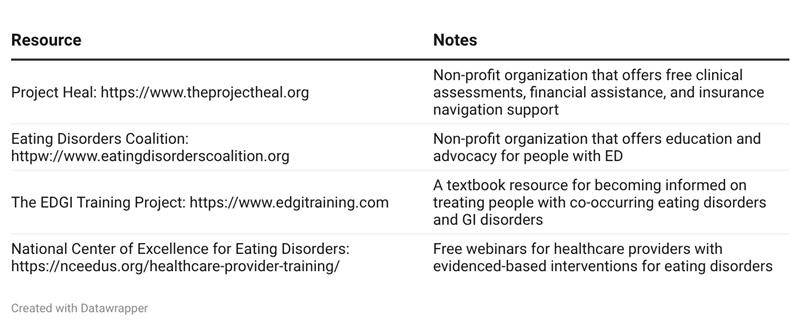
Initiating these conversations with patients can feel uncomfortable, but routine, nonjudgemental inquiry can help direct the patient toward recovery. Table 2 contains resources to share with the patients which they can access for further evaluation and treatment needs.
The necessity of multidisciplinary care
ED treatment requires a multidisciplinary team specialized in EDs, typically a physician, registered dietitian, psychologist, and psychiatrist. GI physicians play a crucial role in identification, diagnostic testing to rule out other causes of symptoms, symptom management, and support recovery. For patients how often experience stigma and shame in health care settings, an ED-aware, trauma-informed GI provider can make an important difference in the recovery journey.
Ms. Rosen is affiliated with Beth Rosen Nutrition and Oshi Health. Dr. Shapiro is affiliated with Gentle GI, PLLC, and the Medical Clinic of Houston, Texas.
The authors reported having no conflicts of interest.
References
Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. 2020;395(10227):899-911. doi:10.1016/S0140-6736(20)30059-3
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed, text rev. American Psychiatric Association; 2022.
National Eating Disorders Association. Eating disorder statistics. Accessed February 17, 2026. https://www.nationaleatingdisorders.org/statistics/#general-eating-disorder-statistics
Bryant E, Spielman K, Le A, et al; National Eating Disorder Research Consortium. Screening, assessment and diagnosis in the eating disorders: findings from a rapid review. J Eat Disord. 2022;10(1):78. doi:10.1186/s40337-022-00597-8
Boyd C, Abraham S, Kellow J. Psychological features are important predictors of functional gastrointestinal disorders in patients with eating disorders. Scand J Gastroenterol. 2010;45(3):307-315.
Norris ML, et al. Gastrointestinal complications associated with anorexia nervosa: a systematic review. Int J Eat Disord. 2016;49(3):216-237.
Mehler PS, Rylander M. Bulimia nervosa—medical complications. J Eat Disord. 2015;3:12.
Puhl RM, Suh Y. Health consequences of weight stigma: implications for obesity prevention and treatment. Curr Obes Rep. 2015;4:182-190.
Burton Murray H, Riddle M, Rao F, et al. Eating disorder symptoms, including avoidant/restrictive food intake disorder, in patients with disorders of gut-brain interaction. Neurogastroenterol Motil. 2022;34(8):e14258. doi:10.1111/nmo.14258
Zickgraf HF, Ellis JM. Initial validation of the Nine Item Avoidant/Restrictive Food Intake Disorder screen (NIAS). Int J Eat Disord. 2018;51(6):580-585.
Santonicola A, Gagliardi M, Guarino MPL, et al. Eating disorders and gastrointestinal diseases. Nutrients. 2019;11(12):3038. doi:10.3390/nu11123038
Satherley R, Howard R, Higgs S. Disordered eating practices in gastrointestinal disorders. Appetite. 2015;84:240-250. doi:10.1016/j.appet.2014.10.006
Chey WD, Hashash JG, Manning L, Chang L. AGA clinical practice update on the role of diet in irritable bowel syndrome: expert review. Gastroenterology. 2022;162(6):1737-1745.e5. doi:10.1053/j.gastro.2021.12.248
Moshiree B, et al. AGA clinical practice update on evaluation and management of belching, abdominal bloating, and distention: expert review. Gastroenterology. 2023;165(3):791-800.e3.
Chiarioni G, Bassotti G, Monsignori A, et al. Anorectal dysfunction in constipated women with anorexia nervosa. Mayo Clin Proc. 2000;75(10):1015-1019. doi:10.4065/75.10.1015
Gomez F, Kilpela LS, Middlemass KM, Becker CB. Sexual trauma uniquely associated with eating disorders: a replication study. Psychol Trauma. 2021;13(2):202-205. doi:10.1037/tra0000586
Staller K, Abber SR, Burton Murray H. The intersection between eating disorders and gastrointestinal disorders: a narrative review and practical guide. Lancet Gastroenterol Hepatol. 2023;8(6):565-578. doi:10.1016/S2468-1253(22)00351-X
Smith J, Arkin E, Rosen B, et al. Comprehensive Nutrition Therapy for Co-Occurring Gastrointestinal & Eating Disorders. Gatekeeper Press; 2025