High endoscopist adenoma detection rate (ADR) is known to reduce post-colonoscopy colorectal cancer (PCCRC) risk within three years, but new findings presented at Digestive Disease Week® (DDW) 2026 suggest this protective effect extends beyond four years.
In an analysis of more than 420,000 quality-assured baseline colonoscopies from the Dutch fecal immunochemical test–based screening program, individuals examined by endoscopists in the lowest four ADR quintiles had roughly two- to threefold higher PCCRC risk beyond four years compared with those examined by endoscopists in the highest ADR category.

In an interview with GI & Hepatology News, presenting author Nanette van Roermund, a research associate and PhD candidate at Amsterdam University Medical Center, said that data on longer-term colorectal cancer risk following high-quality colonoscopy — reflected by ADR and proximal serrated polyp detection rate (PSPDR) — have been limited. “Cancers diagnosed more than four years after colonoscopy have often been assumed to represent newly developed polyps rather than missed polyps,” she added, consistent with the World Endoscopy Organization's (WEO) position.
“Using 10-year follow-up data, our study demonstrates that high-quality colonoscopy is also protective against post-colonoscopy colorectal cancer in the long term, suggesting that cancers arising after four years may still be attributable to missed polyps,” van Roermund remarked. “This underscores the importance of maintaining high procedural quality and routinely monitoring ADR and PSPDR to ensure optimal patient care.”
Study details
Quality-assured baseline colonoscopies from the Dutch screening program from 2014 to 2023 were analyzed. The data set was linked to polyp and colorectal cancer records from the national pathology database, with follow-up available through March 2025. ADR was calculated for each endoscopist who performed at least 75 procedures. To limit surveillance bias, only individuals whose endoscopist recommended a return to screening after 10 years were included.
The primary analysis included individuals with at least four years of follow-up, with time to event measured from the four-year landmark. The association between ADR and PCCRC risk was assessed using a shared frailty Cox proportional hazards model, adjusting for patient age and sex and including endoscopist as a random effect. For subgroup analyses, endoscopists were grouped into quintiles based on ADR. The timing of PCCRC was evaluated among individuals with at least eight years of follow-up within a 10-year period, using 2.5-year intervals.
Risk by ADR
In total, 420,356 colonoscopies were included in the analysis of ADR and PCCRC risk, performed by 521 endoscopists (median ADR, 61.3%). A total of 1,013 PCCRCs were identified over the 10-year period, corresponding to an incidence of 4.42 per 10,000 person-years of follow-up. Among the individuals recommended to return to screening after 10 years (n = 188,730), 138 PCCRCs were detected beyond four years after baseline (4.35 per 10,000 person-years of follow-up), with a median follow-up of seven years.
A significant association was observed between endoscopist ADR and PCCRC risk beyond four years (hazard ratio [HR], 0.97).
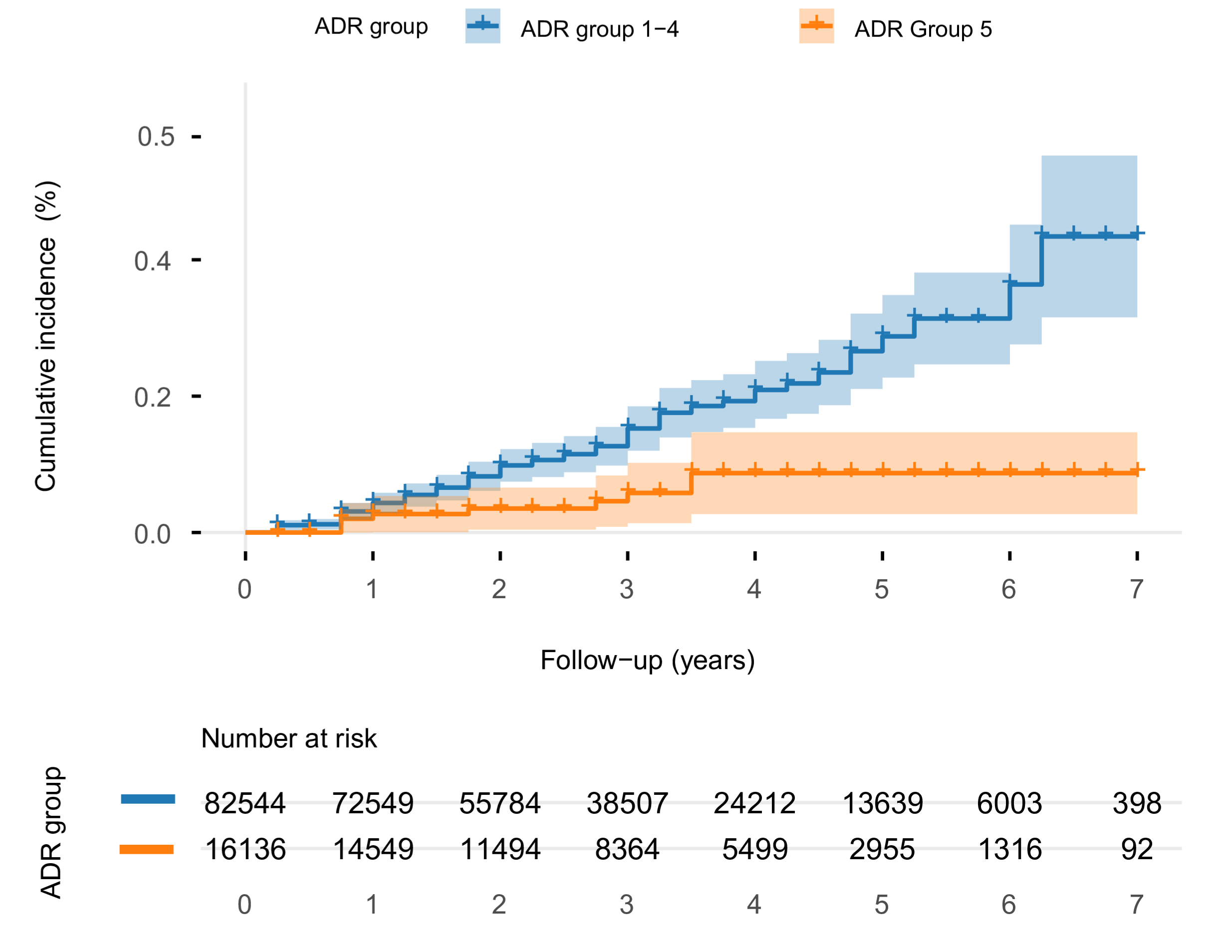
Compared with individuals examined by endoscopists in the highest ADR category (> 66.8%), those examined by endoscopists in categories 1 through 4 were found to have significantly higher PCCRC risk beyond four years, with HRs of 3.30, 2.52, 3.16, and 2.78, respectively.
Among individuals with eight years of follow-up, 171 PCCRCs were detected: 19% occurred within the first 2.5 years, 30% between 2.5 and 5 years, 36% between 5 and 7.5 years, and 15% in the final 2.5 years. Of note, PCCRCs were evenly distributed across the 10-year time frame without early clustering or late increase, the researchers wrote.
Considering all these data, van Roermund stated in the interview, “The key finding of this study is that a high ADR and PSPDR of the endoscopist remain associated with a reduced risk of post-colonoscopy colorectal cancer even beyond four years after colonoscopy.”
She continued, “A limitation of our study is the lack of data on the molecular characteristics of post-colonoscopy colorectal cancers. Future research should focus on evaluating the molecular origins of these cancers to further improve understanding and prevention strategies.”
The author reported having no disclosures.
DDW is AGA's annual meeting, jointly sponsored by AGA, AASLD, ASGE, and SSAT. Learn more at ddw.org.