Editor's note

The incidence of pancreatic cysts has increased over the last decade due to ease of obtaining cross-sectional imaging and a growing older population. Management of these cysts are dependent on the type of pancreatic cyst, associated risk factors, and shared decision-making between the patient and physician(s).
Dr. Vanessa Shami, along with Drs. Ross Buerlein and Himesh Zaver, review the different types of pancreatic cysts in a comprehensive case-based approach. They describe characteristic cyst findings on cross-sectional and endoscopic sonographic imaging, fluid analysis results, and management.
Judy A Trieu, MD, MPH
Editor-in-Chief
The New Gastroenterologist
Introduction

The incidence of pancreatic cystic lesions is increasing, driven in part by an aging population and the widespread use of cross-sectional imaging. The prevalence of pancreatic cysts increases with age, with recent meta-analyses demonstrating a range from 9% in individuals aged 50 to 59 years to as high as 38% in patients aged 80 years or older.1-3
Pancreatic cysts represent a heterogenous group of lesions, and their malignancy potential varies based on cyst type. These lesions are typically divided into two categories: inflammatory fluid collections and pancreatic cystic neoplasms (PCNs).
Inflammatory fluid collections arise as a complication of pancreatitis or pancreatic injury and lack a true epithelial lining. They can be challenging to distinguish from PCNs based on imaging alone. According to the Revised Atlanta Classification, these include acute peripancreatic fluid collections and pseudocysts arising after interstitial pancreatitis, as well as acute necrotic collections and walled-off pancreatic necrosis following necrotizing pancreatitis. Pseudocysts and walled-off pancreatic necrosis generally mature approximately four weeks after pancreatitis onset, though time to "maturity" can be variable.4
PCNs are divided into mucinous and non-mucinous lesions. Mucinous lesions are considered pre-malignant and are characterized by a mucin-secreting columnar epithelium, as seen in intraductal papillary mucinous neoplasms (IPMNs), mucinous cystic neoplasms (MCNs), and solid pseudopapillary neoplasms. In contrast, serous cystadenomas (SCAs) are benign, non-mucinous lesions composed of multiple small cysts lined by cuboidal epithelium and are thought to arise from pancreatic acinar cells. Less common serous lesions include solid serous adenomas, cystic neuroendocrine tumors, and cystic lesions associated with von Hippel-Lindau syndrome.
High-resolution cross-sectional imaging with contrast enhanced computed tomography (CT) or magnetic resonance imaging (MRI) allows for non-invasive assessment and characterization of pancreatic cystic lesions. Endoscopic ultrasound (EUS) is more invasive but provides superior spatial resolution and diagnostic cyst sampling. EUS-directed fine needle aspiration (EUS-FNA) can aid in differentiating serous from mucinous lesions. Mucinous fluid is typically more viscous and may demonstrate a positive "string sign" (a drop of fluid is placed between two glass slides or gloved fingers which are slowly pulled apart, resulting in a string >3.5 mm in length), which has been reported to have a specificity of approximately 95% for mucinous lesions.3,5
The columnar epithelium of mucinous lesions secretes carcinoembryonic antigen (CEA), resulting in mucinous lesions typically having an elevated CEA level >192 ng/mL.6 More recent data have shown that a low cyst fluid glucose level (<50 mg/dL) has a significantly higher sensitivity for identifying a mucinous lesion when compared to CEA alone.7 Cyst fluid amylase level is often elevated in lesions with a connection to the pancreatic duct, which can be seen in IPMNs and pseudocysts. The 2024 international consensus guidelines on pancreatic cysts recommend consideration of molecular DNA markers in cases with diagnostic uncertainty, representing the first major guideline to formally address the role of next generation sequencing in cyst evaluation.8 Microbiopsy forceps, passed through a 19-guage needle, can be utilized to sample the cyst epithelium, improving diagnostic accuracy with a slight increased risk of post-procedure pancreatitis and bleeding.9 Lastly, confocal laser endomicroscopy, performed through a 19-guage needle following intravenous injection of fluorescein, allows real time assessment of the cyst epithelium and may further enhance diagnostic accuracy, although its use remains limited to select centers.10
Case 1
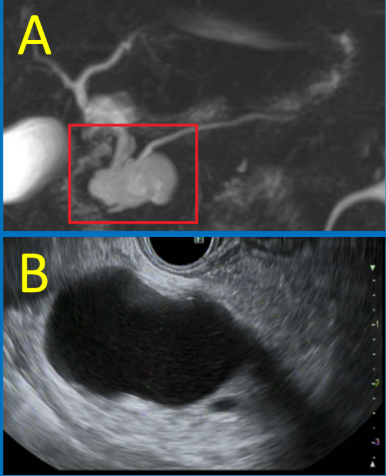
An 81-year-old male was incidentally found on MRI to have a 4.3 cm x 2.1 cm cystic lesion in the head of the pancreas without upstream pancreatic duct dilation (Figure 1A). He was functionally independent and overall healthy for his age. EUS confirmed no other high-risk features such as mural nodules, solid components, or main pancreatic duct dilation (Figure 1B). Cyst fluid aspiration revealed an amylase level of 156 U/L, glucose of 20 mg/dL, and CEA of 139,340 ng/mL. Cytology evaluation supported the presence of mucin but no malignant cells.
Case 1 answer: Branch duct intraductal papillary mucinous neoplasms
Branch-duct intraductal papillary mucinous neoplasms (BD-IPMNs) are the most common PCNs. BD-IPMNs occur with similar frequency in men and women, and may present as solitary or multifocal lesions. By definition, all IPMNs communicate with the pancreatic duct, resulting in elevated cyst fluid amylase. Their columnar epithelium secretes carcinoembryonic antigen (CEA), leading to elevated cyst fluid CEA levels (>182ng/mL[VS), while cyst fluid glucose is typically low (<50 mg/dL).7
Management of BD-IPMNs is guided by the presence of “high-risk” features, which vary slightly among guidelines but generally include3,6,8,11-13:
Malignant or dysplastic cytology
IPMN-related symptoms (pain, jaundice, pancreatitis)
Cyst size ≥3 cm
Enhancing mural nodule or solid component
Main pancreatic duct dilation ≥5 mm
Elevated serum CA 19-9
Rapid cyst growth (definitions range from ≥2.5 mm/year to ≥5 mm over 2 years)
When high-risk features are present, multidisciplinary discussion is recommended to determine the need for further assessment with EUS or surgical resection. In their absence, surveillance is advised, with imaging intervals determined by cyst size. If lesions are unchanged after 5 years, consideration to discontinue surveillance could be given. Patients who undergo surgical resection require ongoing imaging due to the risk of metachronous IPMNs and cancers.
EUS-guided fine needle injection of chemotherapy for ablation of mucinous pancreatic cystic lesions may also be offered in cases with high-risk features. While initial chemoablation incorporated ethanol, a prospective randomized controlled trial demonstrated that elimination of ethanol significantly reduced adverse events, particularly pancreatitis, without compromising efficacy.14 Subsequent studies using ethanol-free protocols have shown that approximately 65%–70% of patients undergoing EUS-guided chemotherapy ablation achieve >95% cyst volume reduction on follow-up imaging, with the vast majority maintaining that response after many years of follow-up.15,16 Despite complete cyst resolution, continued radiographic surveillance is recommended following ablation. This outpatient procedure offers a less invasive alternative to major pancreatic surgery, including pancreaticoduodenectomy, with substantially lower procedural risk and no demonstrated adverse impact on quality of life compared with surgical management.15,16
Case 2
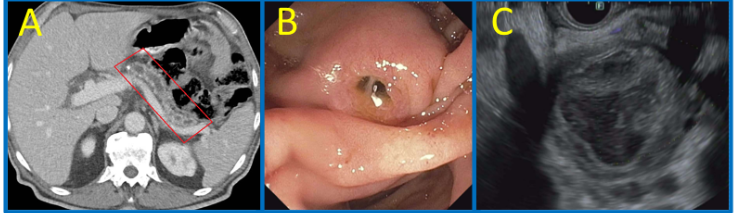
A 68-year-old male presented with new-onset jaundice and elevated bilirubin (total bilirubin 3.3 mg/dL). CT demonstrated a 4.8 cm cystic lesion in the head of the pancreas communicating with the main pancreatic duct, with associated main duct dilation to 9 mm and common bile duct dilation to 15 mm (Figure 2A). He subsequently underwent EUS which revealed mucin extruding from the pancreatic os, consistent with the classic "fish eye" appearance of mucorrhea (Figure 2B). A thick walled, mucin filled cystic lesion was visualized in the pancreatic head, communicating with a dilated, mucin filled main pancreatic duct (Figure 2C).
Case 2 answer: Mixed type IPMN
The patient subsequently underwent pancreaticoduodenectomy, and pathology revealed a mixed type IPMN with a focus of invasive adenocarcinoma. IPMNs are classified into three subtypes: main duct (MD-IPMN), branch duct (BD-IPMN), and mixed type. MD-IPMNs arise from the epithelium of the main pancreatic duct, leading to ductal dilation and a substantially higher risk of malignancy compared with BD-IPMNs. Surgical series report underlying malignancy in up to 60% of resected MD-IPMNs; accordingly, most guidelines recommend multidisciplinary with strong consideration of surgical resection when the main pancreatic duct measures ≥5 mm, and particularly ≥10 mm, in patients with suspected mixed type or MD-IPMN.3,15 In this case, the presence of mucous extruding from the pancreatic os is pathognomonic for a main duct IPMN.
Case 3
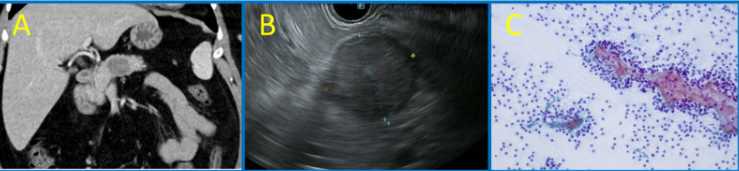
A 37-year-old woman presented with a three-year history of intermittent right upper quadrant abdominal pain, chronic diarrhea, and episodic nausea and vomiting. CT revealed a 3.2 × 2.5 cm hypodense lesion in the pancreatic body with internal septations, concerning for a cystic neoplasm (Figure 3A).
She subsequently underwent EGD and EUS, which revealed a solid appearing, round, well-defined 29 x 28 mm mass in the body of the pancreas (Figure 3B). Cytology from fine needle aspiration showed papillary clusters of uniform cells with nuclear beta catenin and focal synaptophysin positivity. (Figure 3C).
Case 3 answer: Solid pseudopapillary neoplasm
Solid pseudopapillary neoplasms (SPNs) are rare pancreatic tumors that predominantly affect women in their second and third decades of life.11 Patients may present with nonspecific symptoms such as abdominal pain, nausea, vomiting, or weight loss, although many lesions are discovered incidentally on imaging. SPNs typically appear as well-circumscribed, mixed solidandcystic lesions that may arise anywhere within the pancreas, usually as solitary masses.3
Histologically, SPNs are lined by cuboidal epithelial cells and lack communication with the pancreatic duct, resulting in normal cyst fluid amylase levels. Immunohistochemical staining is characteristically positive for beta-catenin, vimentin, alpha-1antitrypsin, and synaptophysin.17 The histogenesis of SPNs remains uncertain, with acinar, endocrine, ductal, and multipotent progenitor cells all proposed as potential cells of origin.
Although SPNs generally exhibit indolent behavior, malignant transformation can occur, with higher risk in larger lesions, particularly those measuring 5 cm or greater. Given their occurrence in younger patients and the potential for progression, surgical resection is typically recommended.3
Case 4
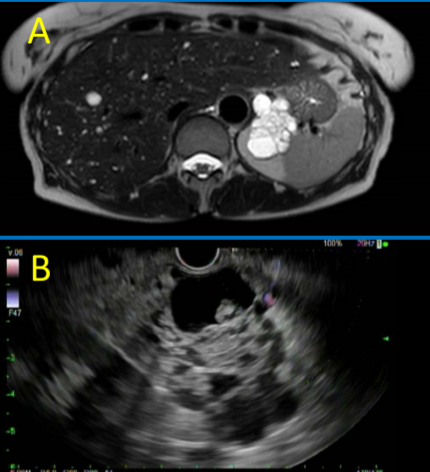
A 68-year-old woman presented with abdominal pain. A CT scan was obtained which incidentally revealed an undifferentiated pancreatic lesion. The pain subsided with antacids. Outpatient MRI demonstrated a multicystic lesion in the pancreatic tail with enhancing internal septations and no definite communication with the main pancreatic duct (Figure 4A). EUS revealed a 43 mm × 38 mm, anechoic, multicystic, septated lesion at the pancreatic body/tail junction (Figure 4B). The lesion contained numerous thin septations without a solid component or mural nodule and did not appear to communicate with the main pancreatic duct.
Case 4 answer: Serous cystadenomas
Serous cystadenomas (SCAs) are typically asymptomatic and most commonly occur in women in their fifth to seventh decades of life.3,11,18,19 Imaging usually reveals a solitary, well-circumscribed microcystic lesion with a characteristic honeycomb pattern. A central stellate scar with "sunburst" calcification is considered pathognomonic, though it appears in only about 20%-30% of cases.11 A less common macrocystic form exists and can be challenging to differentiate from mucinous cystic lesions, as illustrated in this case.
Multifocal SCAs are associated with von Hippel–Lindau (VHL) syndrome and may include a neuroendocrine component. Because SCAs do not communicate with the pancreatic duct, cyst fluid amylase levels are typically low. Diagnosis can often be established on imaging alone, though EUS is helpful when imaging findings are indeterminate. When aspirated, cyst fluid is characteristically thin and serous, with a typically very low CEA level (<5 ng/mL) and often glucose >50 mG/dL.
SCAs have an extremely low risk of malignant transformation (approximately 0.1%).18,19 As such, surgical resection is generally reserved for patients who develop symptoms such as pain or compression of adjacent structures.3,18,19
Emerging technologies
Surgical management of pre-malignant pancreatic cystic lesions is a major undertaking, particularly for patients who require a pancreaticoduodenectomy. As such, it is critical to understand the malignant potential of an individual cyst and balance that with the potential risks and benefits of any intervention. EUS-directed pancreatic cyst ablation has emerged as a less invasive therapeutic option for select premalignant pancreatic cystic neoplasms, particularly in patients who are poor surgical candidates or who wish to avoid major surgery.
Multiple EUS-directed ablation techniques have been studied, with newer approaches demonstrating improved efficacy and lower rates of adverse events. These include chemotherapy ablation (in which cyst contents are aspirated and a chemotherapeutic agent such as paclitaxel with or without gemcitabine is instilled) and radiofrequency ablation. Reported rates of complete cyst ablation vary widely across studies, highlighting the need for further investigation into patient selection, cyst size and morphology, number of ablation sessions, and chemotherapeutic dosing strategies.
Ross C. D. Buerlein, MD; Himesh B. Zaver, MD; and Vanessa M. Shami, MD, are affiliated with the Division of Gastroenterology and Hepatology at the University of Virginia Health System in Charlottesville, Virginia.
Dr. Buerlein is an Assistant Professor of Medicine in the Division of Gastroenterology & Hepatology, Section of Interventional Endoscopy, at the University of Virginia Medical Center in Charlottesville, Virginia.
Dr. Zaver is with the Division of Gastroenterology & Hepatology at the University of Virginia Medical Center in Charlottesville, Virginia.
Dr. Shami is a Professor of Medicine, Director of Endoscopic Ultrasound, and Section Head of Interventional Endoscopy in the Division of Gastroenterology & Hepatology at the University of Virginia Medical Center in Charlottesville, Virginia.
References
Vilela A, Quingalahua E, Vargas A, et al. Global prevalence of pancreatic cystic lesions in the general population on magnetic resonance imaging: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. Published online February 28, 2024. doi:10.1016/j.cgh.2024.02.018
de Oliveira PB, Puchnick A, Szejnfeld J, Goldman SM. Prevalence of incidental pancreatic cysts on 3 tesla magnetic resonance. PLoS One. 2015;10(3):e0121317. doi:10.1371/journal.pone.0121317
Buerlein RCD, Shami VM. Management of pancreatic cysts and guidelines: what the gastroenterologist needs to know. Ther Adv Gastrointest Endosc. 2021;14:26317745211045769. doi:10.1177/26317745211045769
Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102-111. doi:10.1136/gutjnl-2012-302779
Bick BL, Enders FT, Levy MJ, et al. The string sign for diagnosis of mucinous pancreatic cysts. Endoscopy. 2015;47(7):626-631. doi:10.1055/s-0034-1391484
Oh SH, Lee JK, Lee KT, Lee KH, Woo YS, Noh DH. The combination of cyst fluid carcinoembryonic antigen, cytology, and viscosity increases the diagnostic accuracy of mucinous pancreatic cysts. Gut Liver. 2017;11(2):283-289. doi:10.5009/gnl15650
McCarty TR, Garg R, Rustagi T. Pancreatic cyst fluid glucose in differentiating mucinous from nonmucinous pancreatic cysts: a systematic review and meta-analysis. Gastrointest Endosc. 2021;94(4):698-712.e6. doi:10.1016/j.gie.2021.04.025
Ohtsuka T, Fernández-Del Castillo C, Furukawa T, et al. International evidence-based Kyoto guidelines for the management of intraductal papillary mucinous neoplasm of the pancreas. Pancreatology. 2024;24(2):255-270. doi:10.1016/j.pan.2023.12.009
Facciorusso A, Del Prete V, Antonino M, Buccino VR, Wani S. Diagnostic yield of EUS-guided through-the-needle biopsy in pancreatic cysts: a meta-analysis. Gastrointest Endosc. 2020;92(1):1-8.e3. doi:10.1016/j.gie.2020.01.038
Robles-Medranda C, Olmos JI, Puga-Tejada M, et al. Endoscopic ultrasound-guided through-the-needle microforceps biopsy and needle-based confocal laser endomicroscopy increase detection of potentially malignant pancreatic cystic lesions: a single-center study. World J Gastrointest Endosc. 2022;14(3):129-141. doi:10.4253/wjge.v14.i3.129
Elta GH, Enestvedt BK, Sauer BG, Lennon AM. ACG clinical guideline: diagnosis and management of pancreatic cysts. Am J Gastroenterol. 2018;113(4):464-479. doi:10.1038/ajg.2018.14
European evidence-based guidelines on pancreatic cystic neoplasms. Gut. 2018;67(5):789-804. doi:10.1136/gutjnl-2018-316027
Tanaka M, Fernández-Del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017;17(5):738-753. doi:10.1016/j.pan.2017.07.007
Moyer MT, Sharzehi S, Mathew A, et al. The safety and efficacy of an alcohol-free pancreatic cyst ablation protocol. Gastroenterology. 2017;153(5):1295-1303. doi:10.1053/j.gastro.2017.08.009
Lester C, Walsh L, Hartz KM, et al. The durability of EUS-guided chemoablation of mucinous pancreatic cysts: long-term follow-up of the CHARM trial. Clin Gastroenterol Hepatol. 2022;20(2):e326-e329. doi:10.1016/j.cgh.2021.03.041
Moyer MT, Heinle JW, Rhoades SE, Birkholz JH, Peng JS. Successful EUS-guided pancreatic cyst chemoablation safely allows reduction in the frequency of radiographic surveillance: long-term follow-up of randomized prospective data. Gastrointest Endosc. 2024;99(6):962-970. doi:10.1016/j.gie.2023.12.008
Dinarvand P, Lai J. Solid pseudopapillary neoplasm of the pancreas: a rare entity with unique features. Arch Pathol Lab Med. 2017;141(7):990-995. doi:10.5858/arpa.2016-0322-RS
Lee LS, Gardner TB. Pancreatic cysts and pancreatitis in the older adult. Am J Gastroenterol. 2025;120(Suppl 10):S27-S33. doi:10.14309/ajg.0000000000003641.04
Aziz H, Acher AW, Krishna SG, Cloyd JM, Pawlik TM. Comparison of society guidelines for the management and surveillance of pancreatic cysts: a review. JAMA Surg. 2022;157(8):723-730. doi:10.1001/jamasurg.2022.2232