Gastroenterologists in the US are facing mounting pressures to see and scope more patients. The clinical demands of an aging population, together with increased endoscopic volumes driven by the surge in early-onset colon cancer, continue to outpace the available workforce. In response, many health care systems are turning to the GI hospitalist (GIH) model: gastroenterologists hired to work exclusively in the hospital to manage inpatient consultations, perform urgent and emergent endoscopies, coordinate multidisciplinary care, and streamline hospital operations. What began as a pragmatic staffing solution has evolved into a distinct and rewarding career track — one that enriches fellowship training, alleviates key pain points for outpatient colleagues, and enhances institutional performance across both academic and community settings. Institutions that have embraced this model have reaped substantial returns, yet national adoption remains limited. Here is what everyone should know about the GIH model.
Strengthening fellowship training
Academic centers that have implemented the GIH model report meaningful educational benefits. A survey administered to GI fellows across five academic programs found that trainees favored GIH faculty over non-GIH faculty in several domains — including operations and efficiency, teaching and clinical care, and longitudinal feedback — while also endorsing the value of protected inpatient service time maintained by GIH faculty.1 For fellowship programs, the presence of a dedicated inpatient gastroenterologist translates into more structured and predictable teaching, enhanced procedural learning, and improved continuity and quality of care. At the same time, fellows value diversity in clinical experience, preferring a balanced mix of GIH and non-GIH faculty.1 As new endoscopic innovations and technologies continue to emerge, a dedicated GIH embedded in a high-acuity inpatient environment provides the consistent, hands-on foundation that allows trainees to learn, integrate, and confidently apply these advances in their practice.
Benefits to outpatient GI colleagues
GIH faculty have been hired in academic and community practices to help offset the inpatient responsibilities of outpatient gastroenterologists. A nationwide survey of GI program leadership found that reducing time on inpatient service, mitigating burnout, and increasing inpatient quality of care and endoscopy availability were primary motivators for recruiting GI hospitalists.2 By centralizing inpatient responsibilities, outpatient clinicians gain more predictable clinic schedules with fewer interruptions from urgent consults, greater ability to maintain procedural volumes, and improved work-life balance. This redistribution of workload strengthens the entire GI practice and supports long-term faculty satisfaction and retention.
System level benefits: Increased productivity and improved outcomes
Multiple studies now demonstrate significant improvements in efficiency and productivity under a GIH model. At one academic medical center, introduction of a GIH physician with expertise in video-capsule endoscopy and double-balloon enteroscopy (DBE) was associated with increased DBE volumes, higher diagnostic yield for obscure GI bleeding, and more therapeutic interventions.3
Another retrospective study demonstrated a reduction in time to urgent upper endoscopy from 23.8 to 14 hours after transitioning to a GIH model, improving timely care for high-risk patients.4 Finally, a controlled interrupted timeseries analysis across two high-acuity urban academic hospitals showed that adopting a GIH model increased overall weekly inpatient endoscopy volume by 10.9 procedures and outpatient endoscopy volume by 39.8 procedures, despite no change in the number of outpatient endoscopists.5 In other words, the addition of a single GIH generated productivity gains nearly equivalent to hiring a second outpatient gastroenterologist, highlighting the inefficiency of traditional models in which outpatient physicians are routinely pulled in to cover inpatient service. Together, these data show that the GIH model enhances both inpatient and outpatient productivity while improving patient outcomes.
Rewarding and flexible career path
The GIH role has emerged as a personally gratifying and sustainable career path. First and foremost, the GIH model delivers immediately impactful, high-acuity care within a predictable, shift-based schedule. This stands in contrast to the challenges faced by outpatient gastroenterologists, who often manage high clinic volumes, heavy message inboxes, and unpredictable call demands. GIH physicians in academic centers also benefit from meaningful opportunities to teach and mentor trainees.
Importantly, the GIH role offers substantial room for professional growth. GIH physicians can acquire and apply new endoscopic skills with emerging technologies, develop specialized inpatient programs (eg, balloon-enteroscopy services), build multi-disciplinary collaborations, lead quality improvement initiatives, or even craft hybrid roles.
Saad Saffo, MD, assistant professor at Northwestern’s Feinberg School of Medicine, Chicago — who practices as a GIH and attends on inpatient Hepatology and Pulmonary/Critical Care services — illustrates how this model enables meaningful professional expansion. "As the complexity of care for hospitalized patients continues to grow, working as a GI hospitalist has created a space for me to apply my broad training to tailor more practical and individualized solutions for various problems in some of our sickest patients and has inspired ideas for multidisciplinary clinical research and trainee education," Dr. Saffo said. For physicians who thrive at the intersection of high-acuity care, education, and systems-level problem solving, the GIH role provides a uniquely dynamic career path.
Reflecting this growing interest, ASGE now hosts a GI Hospitalist Special Interest Group to develop resources and build a network among those that identify within this bourgeoning practice area.6
Despite its benefits, national adoption of the GIH model remains limited. As of 2023, only 23% of surveyed academic program leaders reported having a GIH at their institution.2 Among programs that lacked GIH physicians, most perceived a lack of benefit from adopting the model.2 This perception likely reflects deeper structural barriers that continue to limit broader implementation. Common barriers include:
A general knowledge gap around the GIH model
Provider preference for outpatient clinical practice
Cultural resistance within practices accustomed to traditional call schedules
Recruitment challenges given novelty of the role and limited supply of fellowship-trained candidates
Funding structures that must accommodate variability in inpatient volumes
Lack of standardized job descriptions across institutions
With thoughtful planning, investment, and alignment among clinical and administrative stakeholders, these barriers are certainly surmountable.
Ideal structuring of the GI hospitalist role
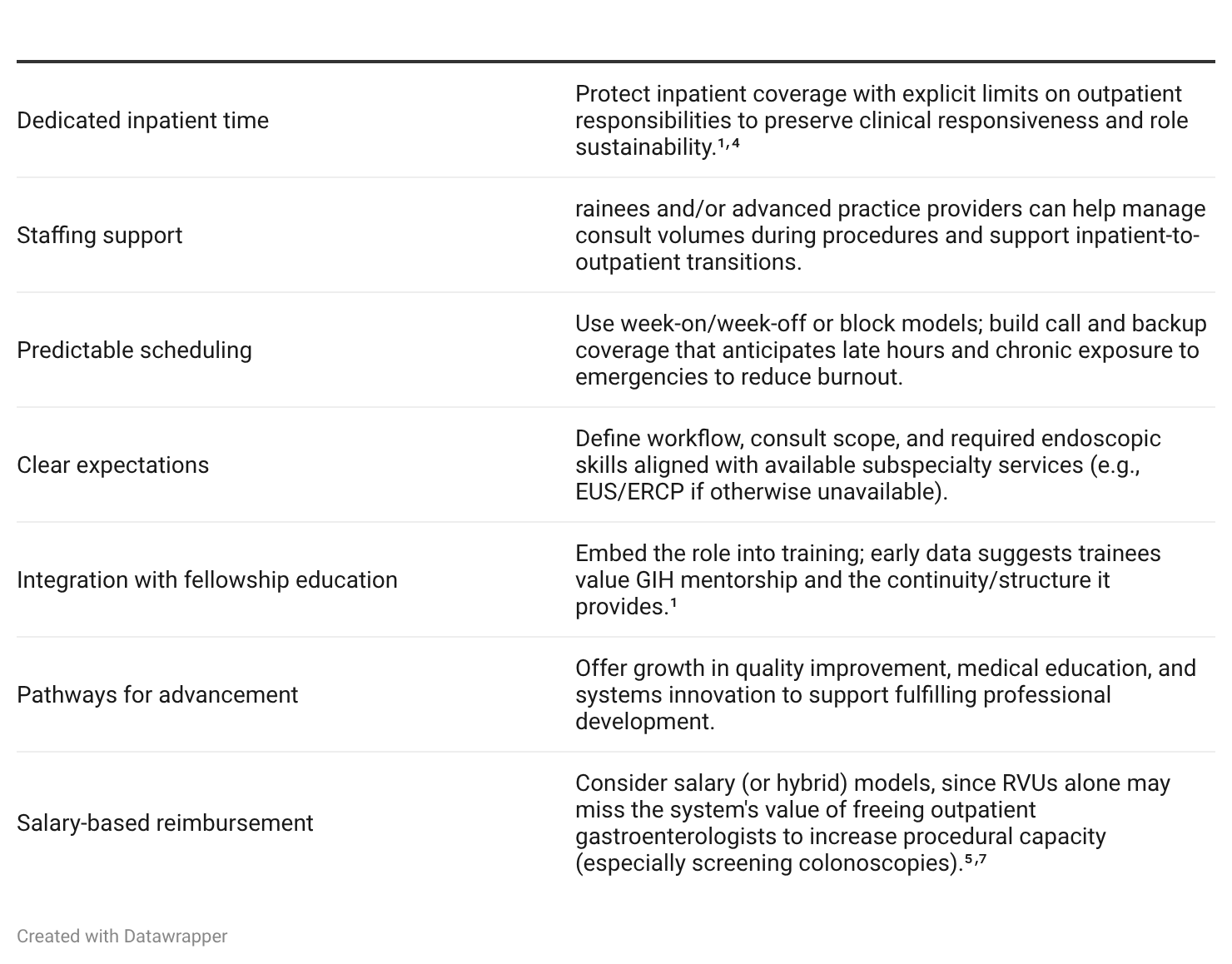
So, what does it take to successfully implement a GIH model? The most important factors include:
Conclusion
The GIH model is a proven, data-driven approach that strengthens fellowship training, improves the work experience of outpatient colleagues, and enhances system-level productivity and patient outcomes. It offers a rewarding and flexible career path for physicians drawn to high-acuity care with interests in education, quality improvement, or systems of innovation.
Although adoption remains variable, the core principles for successful implementation are now well defined, and early adopting practices have demonstrated substantial clinical, operational, and financial benefits. As more health care systems recognize the value of dedicated inpatient expertise — and as interest in the career path continues to grow — the GIH model is poised to play a central role in shaping the future of inpatient gastroenterology.
Vasili Kalas, MD, PhD, is a PGY-6 fellow in the Division of Gastroenterology and Hepatology and member of the Physician-Scientist Training Program at Northwestern University Feinberg School of Medicine, Chicago.
References
Flanagan R, Levine C, Hung K, et al. The educational impact of the GI hospitalist model on gastroenterology fellowship training. Gastroenterology. 2025;168(3):450-453.e2. doi:10.1053/j.gastro.2024.09.028
Flanagan R, Muftah M, Perencevich M, et al. A nationwide survey of gastroenterology program leadership regarding implementation of the GI hospitalist model. Dig Dis Sci. 2023;68(5):1714-1717. doi:10.1007/s10620-022-07763-7
Klein S, Zenger C, Latorre M. The impact of the GI hospitalist model on hospital metrics and outcomes: experience of a large academic medical center. Am J Gastroenterol. 2022;117(10S):e1067-e1068. doi:10.14309/01.ajg.0000862596.05803.8e
Mahadev S, Lebwohl B, Ramirez I, Garcia-Carrasquillo RJ, Freedberg DE. Transition to a GI hospitalist system is associated with expedited upper endoscopy. Presented at: Digestive Disease Week (DDW); 2016
Shung D, Li DK, You K, et al. Adoption of a gastroenterology hospitalist model and the impact on inpatient endoscopic practice volume: a controlled interrupted time-series analysis. iGIE. 2024;3(2):329-332.e2. doi:10.1016/j.igie.2024.04.008
American Society for Gastrointestinal Endoscopy. GI Hospitalist Special Interest Group. Accessed April 15, 2026 https://www.asge.org/home/join-us/asge-special-interest-groups
Latorre M, Gross SA, Pochapin MB. A practical guide to establishing a gastroenterology hospitalist program. Clin Gastroenterol Hepatol. 2021;19(5):871-875.e.2. doi:10.1016j.cgh.2021.02.034