Making computer-aided detection devices available during colonoscopy was associated with higher adenoma detection rates across a large Veterans Health Administration network, according to a cluster-randomized study of more than 334,000 colonoscopies.
Facilities that adopted AI-assisted computer-aided detection during colonoscopy saw adenoma detection rates increase by 4 percentage points, while rates fell slightly at sites that did not use the technology. The findings suggest that making computer-aided detection (CADe) available may improve ADR, a colonoscopy quality metric, in routine VA practice, even among endoscopists with high baseline ADRs.

“Studies have demonstrated that endoscopists with a higher adenoma detection rate protect their patients from colorectal cancer (CRC) incidence and death better than those with a lower adenoma detection rate,” first author Jason A. Dominitz, MD, MHS, of the National Gastroenterology and Hepatology Program at the Veterans Health Administration, Washington, DC, told GI & Hepatology News. “Controlled clinical trials demonstrated that computer-aided detection CADe improves adenoma detection rates (ADR), but this benefit was not clearly demonstrated in real-world studies. Our study is important because we were able to conduct a pragmatic study in a real-world setting that allowed for comparisons of colonoscopy quality with vs without availability of CADe.”
The study, published in Gastroenterology, compared 42 VA facilities that received GI Genius CADe devices with 97 control facilities. Randomized deployment occurred between October 2022 and February 2023, and outcomes were assessed using national administrative, pathology and colonoscopy databases.
The analysis included data from 269 endoscopists at CADe facilities and 547 endoscopists at control facilities. Investigators evaluated 71,594 colonoscopies before and 35,399 after deployment at CADe sites, along with 151,792 predeployment and 75,415 postdeployment procedures at control facilities.
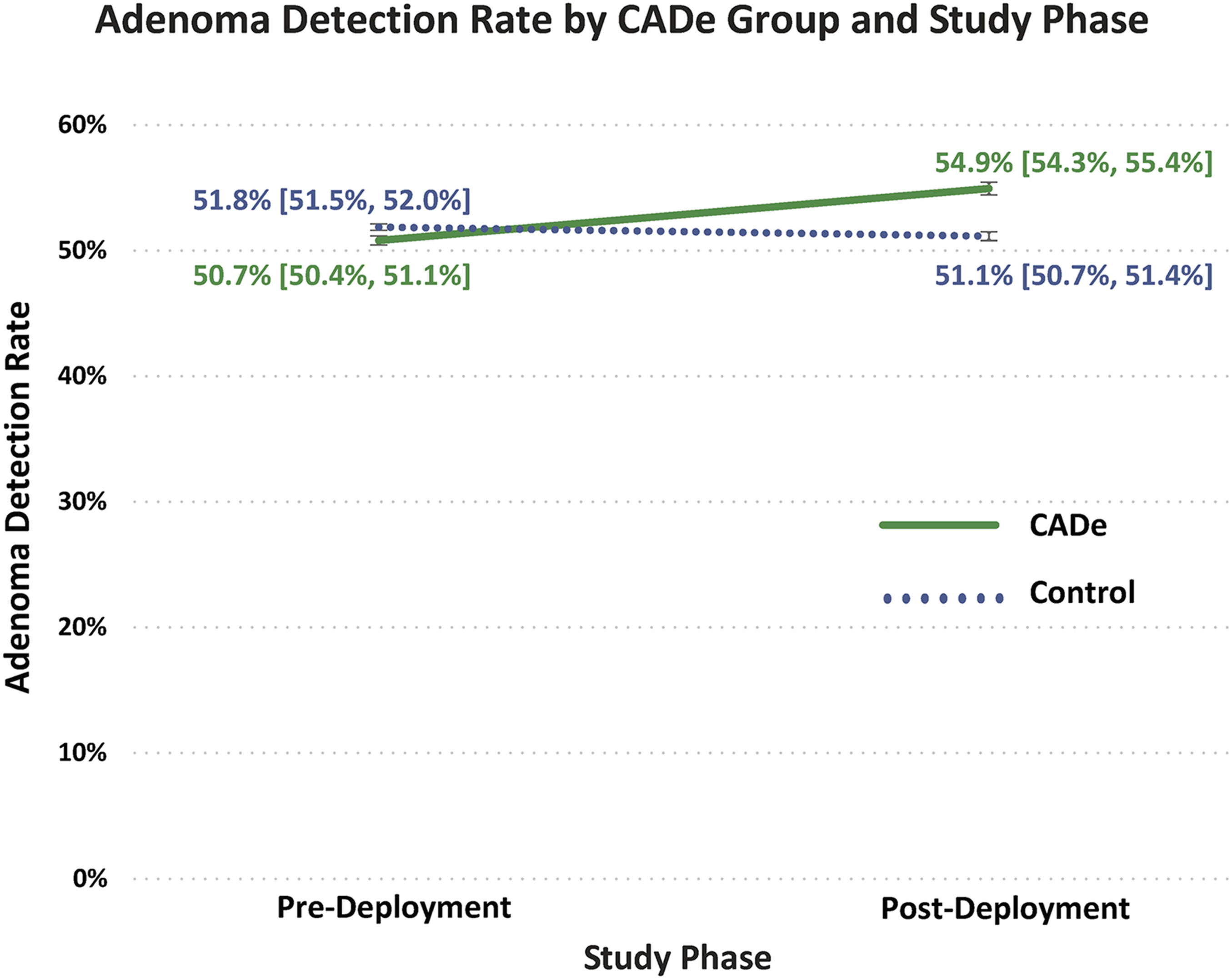
At facilities using CADe, the adenoma detection rate increased from 50.7% before implementation to 54.9% afterward, a gain of 4.2 percentage points. In comparison, control facilities saw a slight decrease in adenoma detection rates, from 51.8% to 51.1% over the same period.
After accounting for differences in patient, physician, and facility characteristics, CADe use was associated with a 22% higher likelihood of detecting an adenoma compared with usual care.
The improvement was seen across endoscopists with a wide range of baseline performance levels. When investigators grouped endoscopists into five categories based on their adenoma detection rates before CADe implementation, they found improvements in every group.
Among endoscopists whose adenoma detection rates were below 40% at baseline, 55% at CADe facilities improved to meet or exceed the 40% benchmark after implementation, compared with 20% of endoscopists at control facilities.
The effect of CADe did not vary by physician specialty, sex, or years of experience. The benefits were also consistent across patient groups defined by sex, race, ethnicity and rural versus urban residence. The only factor that influenced the effect was patient age, with somewhat greater improvements seen in older patients.
In other findings, adenocarcinoma detection rates did not differ significantly between groups. Likewise, after accounting for baseline differences between the groups, CADe use was not associated with improved detection of sessile serrated lesions.
The technology also did not appear to increase false-positive alerts. Rates of non-neoplastic tissue sampling, which the investigators used as a proxy for false positives, were similar between the CADe and control groups after adjustment.
Procedure efficiency also appeared unchanged. In a subset of more than 13,000 colonoscopies with available withdrawal time data, adjusted analyses showed no significant difference in withdrawal times after CADe implementation.
A survey of 124 participating endoscopists found broad acceptance of CADe. Nearly 78% said they liked using the technology, and about three-quarters reported using it in more than 80% of screening and surveillance colonoscopies. Half, however, felt it generated too many false-positive alerts, and one-quarter worried about overreliance on the technology.
The investigators noted several limitations. Because procedure-level CADe usage data and information on colonoscopy indication, polyp size and advanced neoplasia were unavailable, the study could not determine whether higher adenoma detection led to greater detection of advanced lesions or improved long-term colorectal cancer outcomes. In addition, the study population was drawn from the VA and was predominantly male, which may limit generalizability.
The study was funded by the Veterans Health Administration Quality Enhancement Research Initiative. Tonya Kaltenbach, MD, MS, MEd, reported serving as a consultant for Olympus America but the remaining authors reported no relevant conflicts of interest.
Expert Insight
GI & Hepatology News spoke with first author Jason A. Dominitz, MD, MHS, about the study’s findings. He is executive director of the Veterans Health Administration’s National Gastroenterology and Hepatology Program and director of its National Colorectal Cancer Screening Program.
What, if anything, surprised you most about the results?
Dr. Dominitz: Given the large size of the study, and the large number of endoscopists, we were able to assess the association between CADe availability and ADR across a wide spectrum of physicians with respect to their baseline ADR. In other words, we could compare the change in ADR with vs. without CADe for endoscopists with a lower vs a higher ADR before CADe was introduced. I had thought that CADe would be more beneficial for those with lower ADR than for those with higher ADR. Overall, VA endoscopists had a rather high ADR (average around 50%). We found that ADR increased to a similar extent with CADe for all endoscopists. Even those who had a baseline ADR over 65% increased with CADe.
How might the findings influence clinical practice?
Dr. Dominitz: Our findings have already influenced clinical practice throughout the VA, as we used these data (as well as the user survey) to decide to purchase CADe devices for all VA facilities. The VA has approximately 155 endoscopy units that perform about 240,000 colonoscopies each year. VA physicians now have this equipment available to use during colonoscopy.
What gaps remain, and what research should be done next?
Dr. Dominitz: The use of CADe for colonoscopy is relatively new. We don’t know for certain if the improvement in adenoma detection will translate into reductions in CRC incidence and mortality. However, there is good reason to think it might, based on prior research. Some may say that CADe mostly helps find small polyps that are unlikely to progress to cancer. But other research shows that CADe also increases the detection rate for advanced polyps.
There remain questions on how best to integrate use of CADe into the training of endoscopists. Will it lead to training endoscopists to look for green boxes rather than to look for polyps? For experienced endoscopists, might these devices negatively impact endoscopists’ ability to detect precancerous polyps on their own (i.e., deskilling)? It is analogous to installing blind-spot indicators or back-up cameras on cars. Do drivers become too dependent upon these devices, such that if they aren’t available, they may be more accident-prone? But what if the technology itself prevents accidents in the first place?
These are all important points that should be carefully considered.