An international panel of metabolic dysfunction-associated steatohepatitis (MASH) experts reached consensus that noninvasive tests, particularly liver stiffness measurement, may be useful for assessing treatment response in routine clinical practice and could reduce reliance on serial liver biopsies.
The findings, published in Clinical Gastroenterology and Hepatology, come from a modified Delphi consensus study involving 23 experts from 10 countries who evaluated surrogate endpoints for assessing treatment efficacy in MASH across regulatory, reimbursement, and clinical practice settings.
“Given the growing MASH therapeutic landscape, with ongoing phase III trials including semaglutide, survodutide, lanifibranor, pegozafermin, efruxifermin, and resmetirom, among others, defining appropriate surrogate endpoints is increasingly critical,” wrote first author Arun J. Sanyal, MD, of Virginia Commonwealth University, Richmond, and colleagues.
Current regulatory guidelines focus on liver biopsy results, specifically either a one-stage improvement in fibrosis without worsening MASH or resolution of MASH without worsening fibrosis. In the first Delphi survey round, 77% of experts agreed that these biopsy-based measures are still important indicators of treatment effectiveness. At the same time, experts expressed strong support for shifting toward noninvasive tests (NITs) that assess hepatic fibrosis rather than inflammation. Eighty-five percent agreed that NITs are the best way to assess how well treatment is working, and 80% agreed that NITs should replace liver biopsy as the preferred method for measuring treatment outcomes in patients with MASH.
The study used a Delphi process consisting of two survey rounds, supported by a focused review of the published literature. A total of 23 experts in hepatology, gastroenterology, endocrinology, and related specialties participated. Consensus was defined as agreement among at least 75% of panelists, while strong consensus required agreement from at least 95%.
Among the available NITs, liver stiffness measurement (LSM) using vibration-controlled transient elastography (VCTE) or magnetic resonance elastography (MRE) was identified as the leading candidate endpoint. In the second survey round, which focused on clinical practice, 95% of experts agreed that reductions in LSM are an important way to assess treatment effectiveness and may serve as a surrogate marker for long-term outcomes. All panelists agreed that current evidence links lower LSM values with better long-term patient outcomes.
Experts also endorsed specific response thresholds. Specifically, 94% agreed that a 30% decrease or increase in LSM is associated with a corresponding reduction or increase in risk for adverse clinical outcomes. In addition, 82% agreed that a 0.5-point change in the enhanced liver fibrosis (ELF) score has similar value in predicting future clinical outcomes.
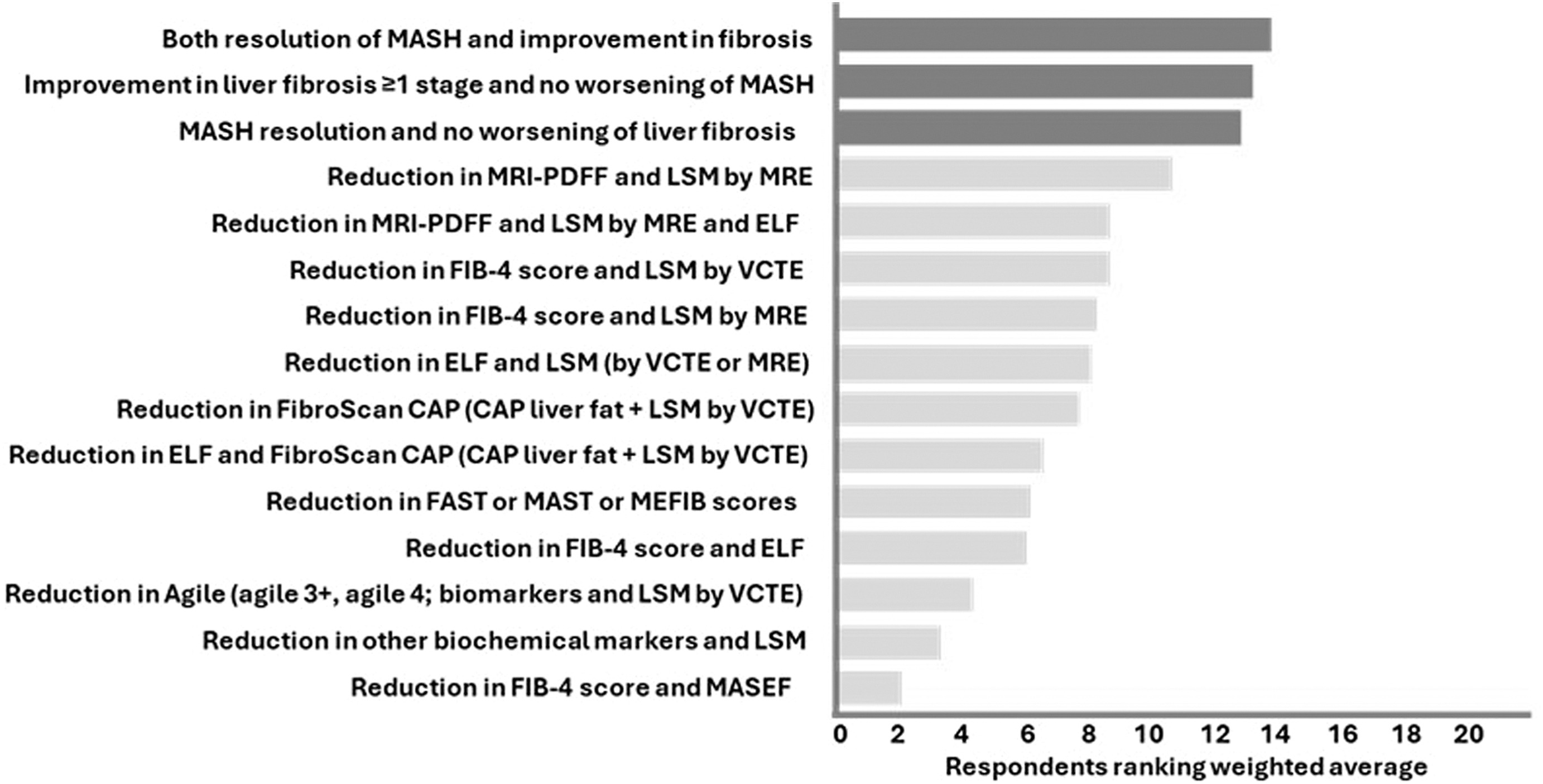
When experts evaluated potential surrogate endpoints, they showed greater support for measures that assess hepatic fibrosis than for markers that reflect disease activity alone. Consensus was reached for both traditional histologic endpoints and a combined imaging endpoint that included reductions in magnetic resonance imaging–proton density fat fraction (MRI-PDFF) and LSM by MRE, with 77% agreement for each. In contrast, several other noninvasive measures—including reductions in the fibrosis-4 (FIB-4) index, FibroScan-aspartate aminotransferase (FAST) score, magnetic resonance imaging–aspartate aminotransferase (MAST) score, magnetic resonance elastography–fibrosis-4 (MEFIB) score, and Agile scores—did not achieve consensus.
“In routine clinical practice, NITs were considered important for assessing treatment effective ness and as potential surrogate outcomes,” the researchers wrote. “Their expanding role underscores the need for clear guidance to facilitate wider implementation. As the therapeutic landscape evolves, periodic reassessment of these tools will be necessary to ensure relevance across treatment contexts.”
The authors noted several limitations, including the lack of direct discussion among panelists inherent to the Delphi process and the reliance on expert opinion rather than head-to-head comparisons of surrogate endpoints. They also emphasized the need for prospective studies to confirm that changes in noninvasive markers predict long-term clinical outcomes before these measures can gain broader regulatory acceptance.
The study was funded by Novo Nordisk. Two coauthors were employed by Novo Nordisk, and multiple authors reported consulting fees, advisory roles, research funding, speaker fees, stock ownership, or other relationships with pharmaceutical and biotechnology companies involved in MASH drug development.

Expert Insight
GI & Hepatology News invited Robert Fontana, MD, professor of medicine and director of the transplant hepatology fellowship program at University of Michigan Health, to weigh in on the study.
Why is this study important?
Dr. Fontana: We need to have quantitative, simple, reliable, and widely available tools in clinical practice to know where we are going in managing individual MASH patients. As the study authors point out, although liver biopsy is the gold standard for clinical trials this does not translate well to clinical practice for several reasons. Firstly, liver biopsy is limited by sampling artifact. It is also invasive, costly, and most patients do not like to undergo serial biopsies. With so many MASH patients, it is also not practical to biopsy everyone.
There are multiple proposed NITs to use for treatment efficacy, and they all have advantages and disadvantages but there is no single NIT to use. This is reflected in the variability of Delphi expert opinion results. MR-based methods (MRID PDff and MRE) are probably the most accurate and reliable. However, they are not widely available outside of major medical centers and are extremely costly and cumbersome. So although perhaps the most accurate, MRI is not currently practical or scalable. LSM using VCTE is more widely available, simple to obtain as POC test, and affordable. However, it is not as accurate as MRI and there are more causes of false positive (alcohol use) and patient factors (high BMI) that are limitations. Lastly, the panel and other experts agree that serum ELF testing and FIB-4 are not well established enough to hang your hat on by themselves.
In clinical practice, most of us use an imaging-based biomarker (MRI or VCTE) in combination with blood biomarkers (transaminases, serum ELF panel) and do not use liver biopsies at all to assess treatment response. So, this paper will likely be cited by practitioners, insurers and other groups regarding “consensus recommendations” on how to monitor treatment and disease progression going forward.
How might the findings influence clinical practice?
Dr. Fontana: The paper provides a relative ranking of various options as seen by an expert panel. Again, insurers, hospitals, and physicians will likely find this useful information to guide their clinical practice, establish practice patterns, and inform equipment purchasing and development of NITs.
What still needs investigation?
Dr. Fontana: There are over 20 new drugs and other approaches being tested for non-cirrhotic and cirrhotic MASH. Most of these ongoing studies are measuring multiple imaging-based and serum-based NITs in addition to liver biopsy. Therefore, we should have a lot of good, prospectively collected data using standardized testing modalities to inform the community in the next few years.
Is there anything else you’d like to say about this work?
Dr. Fontana: Since MASLD is already the leading cause of liver-related morbidity and mortality and the prevalence is continuing to rise, this area is of great importance to all GI doctors throughout the US and worldwide. Therefore, this topic should continue to garner a lot of attention for the next 5 to 10 years as our understanding of the natural history of MASH evolves and new and improved therapies emerge.
Dr. Fontana is a member of the AASLD MASLD Special Interest Group. He also conducts research funded by Fractyl and Takeda and he consults for Roche, Intellius, MasterSwitch, and eGenesis.