Leaving prophylactic pancreatic duct stents in place for four weeks instead of checking for removal after two weeks reduced the need for a repeat endoscopic procedure without increasing pancreatitis or other clinically important complications in patients undergoing endoscopic retrograde cholangiopancreatography (ERCP), according to a multicenter randomized trial.

“This trial provides the first prospective, multicenter randomized evidence that a four-week prophylactic pancreatic duct stent retention interval is safe and significantly reduces the need for endoscopic removal compared to a two-week interval,” the study’s first author, Dong Kee Jang, MD, PhD, of the division of gastroenterology in the department of medicine at Samsung Medical Center, South Korea, told GI & Hepatology News. “It suggests that a more conservative management strategy is viable without increasing the risk of post-ERCP pancreatitis.”
The findings, published in Clinical Gastroenterology and Hepatology, may help settle a long-standing question about how long prophylactic pancreatic duct stents should remain in place after ERCP. Current guidelines disagree: The European Society of Gastrointestinal Endoscopy recommends checking for and removing retained stents within five to 10 days, while the American Society for Gastrointestinal Endoscopy recommends removal within two to four weeks.
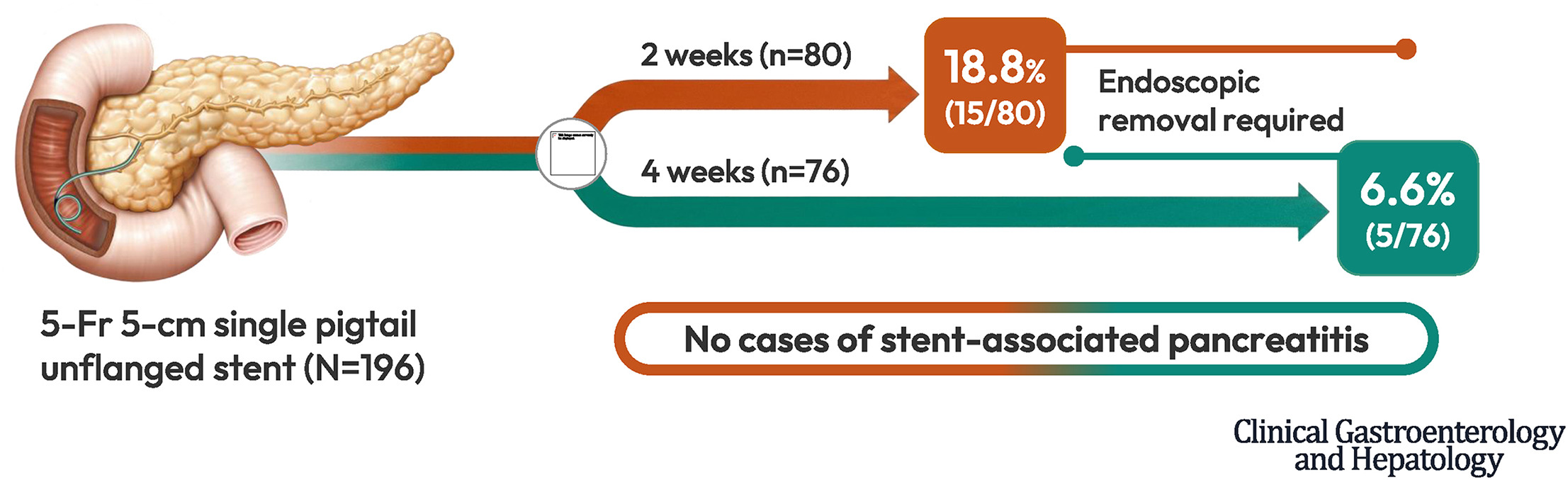
Dr. Jang and colleagues enrolled adults undergoing ERCP at nine tertiary centers in South Korea between July 2021 and March 2024. All patients received the same 5-French, 5-cm, single-pigtail pancreatic duct stent without an internal flange after inadvertent pancreatic duct cannulation during biliary access. Stents were placed to prevent post-ERCP pancreatitis or to facilitate difficult biliary cannulation. Patients were randomly assigned to have an abdominal X-ray two or four weeks after ERCP to determine whether the stent had passed spontaneously. Those with retained stents underwent endoscopic removal.
Of 182 patients screened, 160 were randomly assigned to one of the two follow-up groups. A total of 156 completed follow-up and were included in the analysis. The groups had similar baseline characteristics. The average age was about 62 years, about half of the patients were men, and the most common reason for ERCP was choledocholithiasis. About two-thirds of patients received a pancreatic duct stent to help prevent post-ERCP pancreatitis, while about one-third received a stent to make biliary cannulation easier.
The primary outcome favored the four-week follow-up strategy. Only 7% of patients in the four-week group required endoscopic stent removal, compared with 19% of those in the two-week group. That means about one endoscopic removal procedure was avoided for every eight patients managed with the longer follow-up interval.
The lower rate of endoscopic stent removal was due to more patients passing their stents on their own. By the scheduled follow-up visit, 92% of patients in the four-week group had passed the stent spontaneously, “which exceeded our initial assumptions,” Dr. Jang said, compared with 81% of those in the two-week group.
Importantly, waiting four weeks to assess stent passage did not appear to increase the risk of complications. Post-ERCP pancreatitis occurred in 11% of patients in the four-week group and 15% of those in the two-week group, a difference that was not statistically significant. Most cases were mild. Two patients in each group developed moderate pancreatitis, and no patients developed severe pancreatitis. The median time to pancreatitis onset was one day after ERCP, suggesting that most cases occurred soon after the procedure rather than during the longer period of stent retention.
The investigators found no cases of stent-associated pancreatitis, defined as pancreatitis that developed more than 48 hours after ERCP while the stent was still in place. No patients developed pancreatitis more than two weeks after the procedure or experienced other serious complications requiring emergency care. Hospital stays and postprocedure amylase and lipase levels were also similar between the two groups.
Subgroup analyses showed similar results. Outcomes did not differ between patients who received stents to prevent post-ERCP pancreatitis and those who received stents to help with difficult biliary cannulation. Rates of endoscopic stent removal, spontaneous stent passage, and pancreatitis were similar regardless of the reason for stent placement.
“These findings support shifting to a four-week assessment interval, which can safely reduce unnecessary endoscopic removal procedures and associated health care burdens,” Dr. Jang said.
The authors noted several limitations. All patients were treated at tertiary hospitals in South Korea, so the findings may not apply to other practice settings. The results are specific to the 5-French, 5-cm, single-pigtail pancreatic duct stent without an internal flange used in the study and may not apply to other stent designs. “Additionally, longitudinal studies are needed to further confirm long-term safety regarding rare, late-onset complications,” Dr. Jang said.
The study’s co-corresponding authors were Min Kyu Jung, MD, PhD, and Sang Hyub Lee, MD, PhD.
The researchers reported having no disclosures.

Expert Insight
GI & Hepatology News invited Sumant Inamdar, MD, MPH, an interventional gastroenterologist in the division of gastroenterology and hepatology at the University of Arkansas for Medical Sciences, Little Rock, to comment on the study.
What are the potential clinical implications of the research?
Dr. Inamdar: The main clinical implication is that, for the specific stent studied (a 5-Fr, 5-cm, single-pigtail, unflanged prophylactic pancreatic duct stent), a four-week assessment strategy may be safe and more efficient than routine two-week assessment. Waiting longer increased spontaneous stent passage from 81.3% to 92.1% and reduced the need for endoscopic removal from 18.8% to 6.6%. For patients, this could mean fewer repeat endoscopies, less anesthesia exposure, fewer visits, and lower cost. For endoscopy units, it may reduce avoidable procedures and free capacity for higher-priority therapeutic cases. Importantly, these findings support a selective, stent-specific approach, not a universal 4-week strategy for all pancreatic stents. The results are most applicable to short, unflanged prophylactic stents designed to pass spontaneously, and should not be automatically extrapolated to flanged, longer, therapeutic, or otherwise higher-risk pancreatic duct stents.
What additional research may be needed/what questions remain unanswered?
Dr. Inamdar: Several questions remain. First, the study was performed in tertiary centers in South Korea, so it would be helpful to see whether the same findings hold across other health systems and practice environments. Second, the results are highly dependent on the stent design. Different stent lengths, diameters, flanged stents, or internally anchored stents may have very different migration and retention behavior. Third, the study was not designed to evaluate longer-term pancreatic duct changes after delayed stent passage or retention. Although no stent-associated pancreatitis was observed, the sample size may not be large enough to detect rare adverse events. Additional studies with longer follow-up could help clarify whether prolonged retention has any delayed ductal consequences. Finally, contemporary post-ERCP pancreatitis prevention often includes rectal NSAIDs and protocolized hydration, but rectal NSAIDs were not used in this trial because they were not available in South Korea. That makes the study internally consistent, but it raises the question of how these results translate to centers where rectal indomethacin and other prophylactic strategies are routinely used.
Is there anything else you’d like to say about this work?
Dr. Inamdar: This is a pragmatic and clinically useful study because it answers a question that advanced endoscopists face frequently. Its strength is not only that it is randomized and multicenter, but that it focuses on an outcome that matters to patients and endoscopy units: the need for an additional endoscopic procedure. The findings should encourage guideline committees and endoscopy practices to think more carefully about stent-specific follow-up intervals rather than applying a single removal timeline to all pancreatic duct stents.
Dr. Inamdar reported having no disclosures.