People with lean MetALD had an 82% higher adjusted risk of all-cause mortality than overweight or obese patients with the disease, along with significantly higher risks of major adverse liver outcomes (MALO), according to a large retrospective cohort study published in Clinical Gastroenterology and Hepatology.
“Very little is known about how body weight modifies disease behavior and outcomes within MetALD,” first author Binu V. John, MD, MPH, chief of gastroenterology and hepatology at the Miami VA Healthcare System in Miami, Florida, told GI & Hepatology News. “Our study demonstrates that people with a normal body mass index and MetALD are not a lower-risk group simply because they lack obesity. They carry a substantially higher burden of liver-related complications and death. This has important implications for how we screen, counsel and manage these patients.”
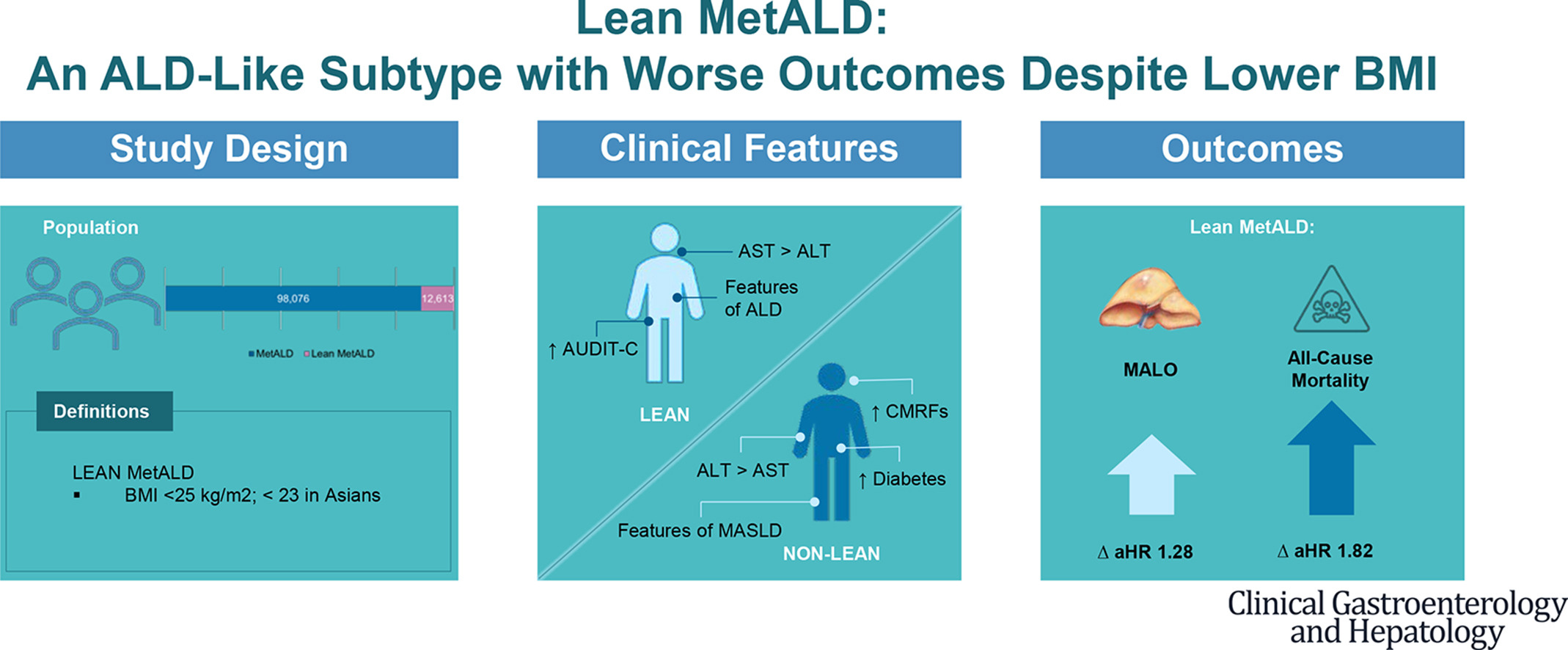
Using data from the Veterans Analysis of Liver Disease (VALID) cohort, Dr. John and colleagues identified 98,076 people with metabolic dysfunction–associated steatotic liver disease with increased alcohol intake (MetALD).
MetALD was defined by hepatic steatosis, harmful alcohol use based on Alcohol Use Disorders Identification Test-Concise (AUDIT-C) scores and at least one of five cardiometabolic risk factors: elevated body mass index (BMI), impaired glucose metabolism or diabetes, hypertension, hypertriglyceridemia, or low HDL cholesterol. Researchers classified 12,613 (12.9%) as lean MetALD, defined as MetALD with a normal BMI — less than 23 kg/m² for people of Asian descent, and less than 25 kg/m² for others.
Primary outcomes were all-cause mortality and MALO, a composite of hepatocellular carcinoma, hepatic decompensation, liver transplantation and liver-related death. Median follow-up was 4.7 years among those with lean MetALD and 5.6 years among those with non-lean MetALD.
Researchers found that individuals with lean MetALD experienced higher rates of hepatic decompensation (7.2% vs. 4.4%) and liver-related death (0.9% vs. 0.4%) than those with non-lean MetALD.
People with lean MetALD also had higher adjusted incidence rates per 1,000 person-years for decompensation (12.1 vs. 8.9), liver-related death (1.2 vs. 0.9), MALO (13.1 vs. 9.7) and all-cause mortality (25.7 vs. 14.2).
In landmark analyses, the adjusted cumulative incidence of MALO at five years was 6.3% among those with lean MetALD and 4.7% among those with non-lean MetALD, while all-cause mortality was 12% and 6.8%, respectively. At 10 years, MALO was 12.3% vs. 9.2%, and all-cause mortality was 22.6% vs. 13.2%.
Lean MetALD was also associated with higher risks of MALO and mortality when excluding people with baseline cirrhosis or advanced fibrosis. Findings were similar when analyses were restricted to people with diabetes or multiple cardiometabolic risk factors.
The study has several limitations. According to the authors, these included the retrospective design, potential residual confounding, reliance on AUDIT-C rather than direct alcohol quantification and a predominantly veteran population, which may limit generalizability. They also acknowledged that excluding events occurring within the first year after steatosis diagnosis may have reduced observed early event rates.
Dr. John reported receiving institutional research support from Exact Sciences, Genentech and Takeda unrelated to this study. No other personal or financial conflicts of interest were reported.

Expert Insight
GI & Hepatology News invited first author Binu V. John, MD, MPH, chief of gastroenterology and hepatology at the Miami VA Healthcare System in Miami, Florida, to elaborate on the study results.
Did any of the study findings stand out?
Dr. John: The most striking finding was the magnitude of the mortality difference. Patients with lean MetALD had an 82% higher risk of all-cause mortality compared with those with non-lean MetALD, even after adjusting for multiple confounders. This was surprising given that lean patients had fewer cardiometabolic risk factors. A second unexpected finding was the higher rate of cardiac deaths in lean MetALD despite fewer traditional cardiovascular risk factors — a paradox that mirrors observations in lean metabolic dysfunction-associated steatotic liver disease (MASLD) and likely reflects unmeasured differences in genetic factors, systemic inflammation, and endothelial function that BMI alone does not capture.
What are the practical implications of these findings for clinicians?
Dr. John: Our findings suggest that clinicians should not be falsely reassured by a normal BMI in a patient with MetALD. When a lean person presents with steatotic liver disease and moderate alcohol use, the predominant driver of liver injury is likely alcohol rather than metabolic syndrome, and the management should reflect that, with a strong focus on alcohol use disorder treatment, including pharmacotherapy and behavioral interventions. In contrast, non-lean MetALD individuals more closely resemble MASLD and should receive aggressive management of their cardiometabolic risk factors. In short, lean MetALD may warrant a treatment approach closer to alcohol-associated liver disease than MASLD.
What are the next steps for research in this area?
Dr. John: First, it would be interesting to understand the biological mechanisms that explain why lean MetALD carries a worse prognosis than non-lean MetALD despite fewer cardiometabolic risk factors. This likely reflects a combination of genetic predisposition, differences in body composition, particularly visceral adiposity that is not captured by BMI alone, and the predominant role of alcohol as the driver of liver injury in lean patients.
Second, we hope to evaluate whether targeted treatment of alcohol use disorder in patients with lean MetALD, including pharmacotherapy with agents, such as naltrexone, acamprosate, or GLP-1 receptor agonists, which have shown promise in reducing alcohol consumption, translates into meaningful improvements in liver-related outcomes and survival. Our research group and others have demonstrated that GLP-1 receptor agonists are associated with a significant reduction in liver-related outcomes and mortality in patients with harmful alcohol use, and it would be interesting to examine whether this benefit is particularly pronounced in the lean MetALD subgroup.