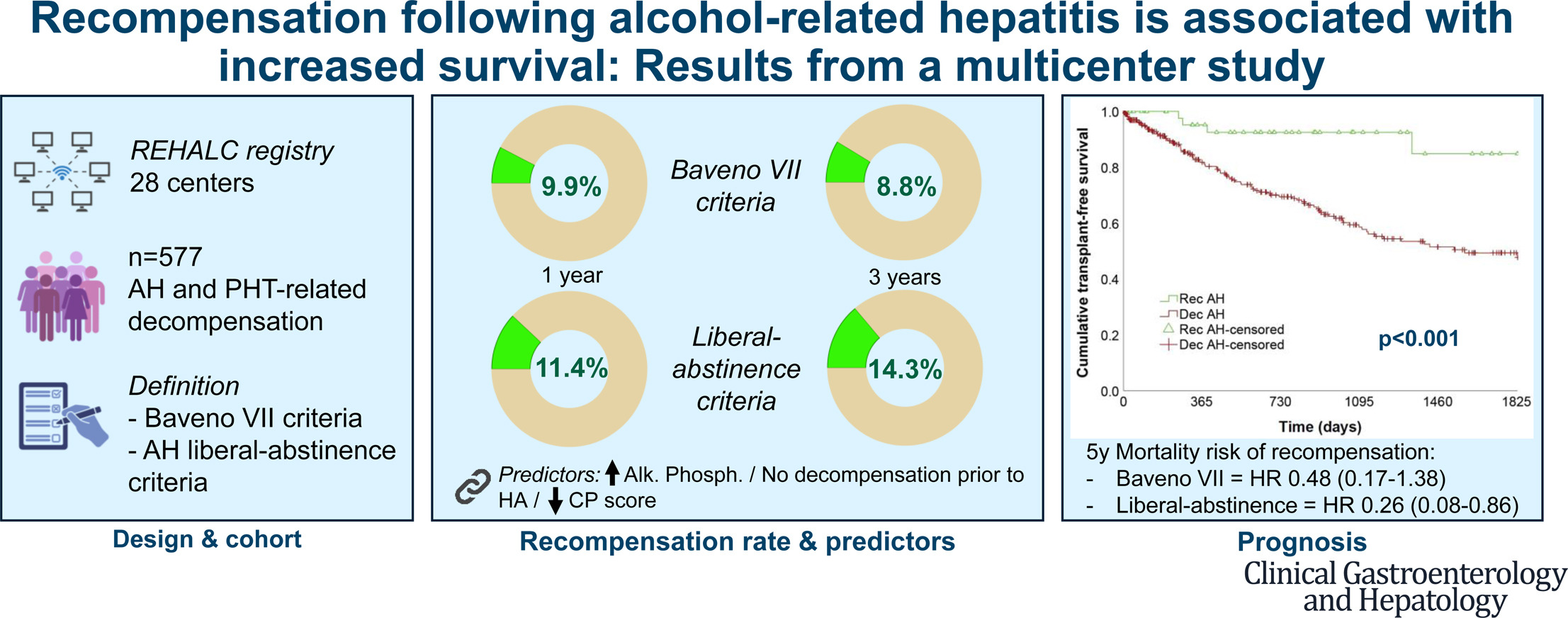
Patients who survived an episode of alcohol-related hepatitis (AH) and subsequently achieved liver disease recompensation had substantially higher long-term transplant-free survival than those who remained decompensated, according to a multicenter study published in Clinical Gastroenterology and Hepatology. Five-year transplant-free survival was 84.9% among patients who achieved recompensation at 1 year compared with 47.7% among patients with persistent decompensation.

“Recompensation after alcohol-related hepatitis is not rare, occurring in ~10–14% of patients overall and up to ~25% among those achieving alcohol abstinence,” lead author Jordi Gratacós-Ginès, MD, PhD, of the Liver Unit at Hospital Clínic Barcelona in Spain told GI & Hepatology News.
Study design
The study, which included 577 patients from Spain, evaluated the rate, predictors and prognostic significance of recompensation after AH among patients enrolled in the REHALC registry across 28 Spanish centers between 2014 and 2021.
The researchers included patients with AH and portal hypertension–related decompensation who were discharged alive after hospitalization. Of 1,101 eligible survivors, 577 met inclusion criteria and were analyzed. Most patients (85%) had cirrhosis at baseline.
Recompensation was assessed using the Baveno VII criteria, which require resolution of decompensating events, improvement in liver function and alcohol abstinence. Researchers also evaluated an adapted “alcohol-related hepatitis liberal-abstinence” definition that removed the abstinence requirement while retaining all other criteria.
Recompensation rates increased with abstinence
Using Baveno VII criteria, 9.9% of patients achieved recompensation at 1 year and 8.8% at 3 years. Under the liberal-abstinence definition, recompensation rates increased to 11.4% at 1 year and 14.3% at 3 years.
“Adapted (liberal-abstinence) criteria may better capture clinically meaningful improvement even in patients who are not completely abstinent from alcohol,” said Dr. Gratacós-Ginès.
Among patients with cirrhosis, recompensation rates were 8.2% at 1 year and 9% at 3 years using Baveno VII criteria. Rates were higher among patients without cirrhosis, reaching 20% at 1 year.
The analysis also examined outcomes among patients who maintained alcohol abstinence. Among 215 patients who were abstinent from alcohol at 1 year, recompensation rates reached 26.5% at 1 year and 25.8% at 3 years.
Factors associated with recompensation
Multivariable analyses identified several factors associated with recompensation. Higher alkaline phosphatase levels, lower Child-Pugh scores and the absence of liver decompensation before the AH episode independently predicted recompensation at 1 year. Specifically, each 10-unit increase in alkaline phosphatase was associated with 1.03 times the odds of recompensation, while each 1-point increase in Child-Pugh score was associated with lower odds of recompensation. Patients with prior decompensation were less likely to achieve recompensation.
At 3 years, higher alkaline phosphatase levels, absence of prior decompensation and shorter duration of alcohol use before developing AH were independently associated with recompensation.
Recompensation linked to improved survival
Clinical status remained dynamic during follow-up. Among 57 patients who had achieved recompensation at 1 year, 11 re-decompensated by year 3 and three died. Conversely, among 332 patients with decompensated AH at 1 year, 17 (5.1%) achieved recompensation at 3 years.
To evaluate prognosis, researchers performed a landmark analysis beginning 1 year after discharge. Recompensation was associated with higher transplant-free survival. At a follow-up time of 5 years, 96 patients with decompensated AH and four patients with recompensated AH had died or undergone liver transplantation.
When the liberal-abstinence criteria were applied, recompensation remained independently associated with a lower risk of death or liver transplantation.
Study limitations
The researchers noted several limitations, including the retrospective design, inability to determine the precise timing of recompensation, loss to follow-up between years 1 and 3, and reliance on patient self-report or family interviews for most alcohol-use assessments. They also acknowledged the lack of biological samples for the analysis of pathophysiological mechanisms of recompensation.
According to Dr. Gratacós-Ginès, “Recompensation should be considered a dynamic and achievable clinical state, particularly in the context of sustained abstinence.”
Implications for clinical practice
According to Dr. Gratacós-Ginès, these data support incorporating recompensation as a relevant therapeutic goal in AH survivors. “These results reinforce the need for structured addiction support and long-term follow-up,” he explained. “Early identification of patients with higher probability of recompensation may help optimize resource allocation, tailor follow-up intensity and inform transplant evaluation timing.”
Dr. Gratacós-Ginès said the findings also suggest that strict application of abstinence-based definitions may underestimate recovery, which has implications for both research and clinical classification.
How the findings might affect patient care
Dr. Gratacós-Ginès pointed out three ways the findings from the study might affect patient care:
Clinicians can provide a more optimistic but realistic prognosis, particularly for patients achieving abstinence.
Recompensation status could be incorporated into risk stratification models and decisions regarding liver transplant listing or delisting.
The concept of recompensation may help improve patient engagement, as it highlights the potential for meaningful recovery.
Next steps for research
“Future studies should prospectively validate predictive models for recompensation, better characterize the temporal dynamics of liver recovery, and, most importantly, explore biomarkers of hepatic repair and regeneration to improve the prediction of recompensation and optimize organ allocation,” concluded Dr. Gratacós-Ginès.
Several authors reported financial relationships, including grants, consulting fees, honoraria, travel support, advisory roles, or speakers’ bureau participation with medical societies and pharmaceutical or medical device companies; the remaining authors reported no conflicts.