Upadacitinib and infliximab showed the fastest early symptom relief among biologic-naive patients with moderate to severe ulcerative colitis, according to a post hoc analysis of individual patient-level data from 11 randomized trials published in Clinical Gastroenterology and Hepatology.
The analysis included 3,573 biologic-naive patients with moderate to severe ulcerative colitis who received standard induction doses of infliximab, adalimumab, golimumab, vedolizumab, ustekinumab, mirikizumab, tofacitinib, upadacitinib, or placebo. Investigators compared early symptom improvement using Patient-Reported Outcome-2 (PRO-2) response, defined as at least a 50% reduction in stool frequency and rectal bleeding scores at week 2. Infliximab was used as the active comparator in adjusted analyses.

“The biggest takeaway is that there’s a clear hierarchy when it comes to how fast these drugs provide symptom relief,” said senior author Neeraj Narula, MD, MPH, FRCPC, of McMaster University, in an interview with GI & Hepatology News. “Upadacitinib and infliximab are the clear frontrunners for rapid onset, showing significant patient-reported improvement by week two, though many other therapies definitely catch up by the end of induction.”
Rapid response favored upadacitinib and infliximab
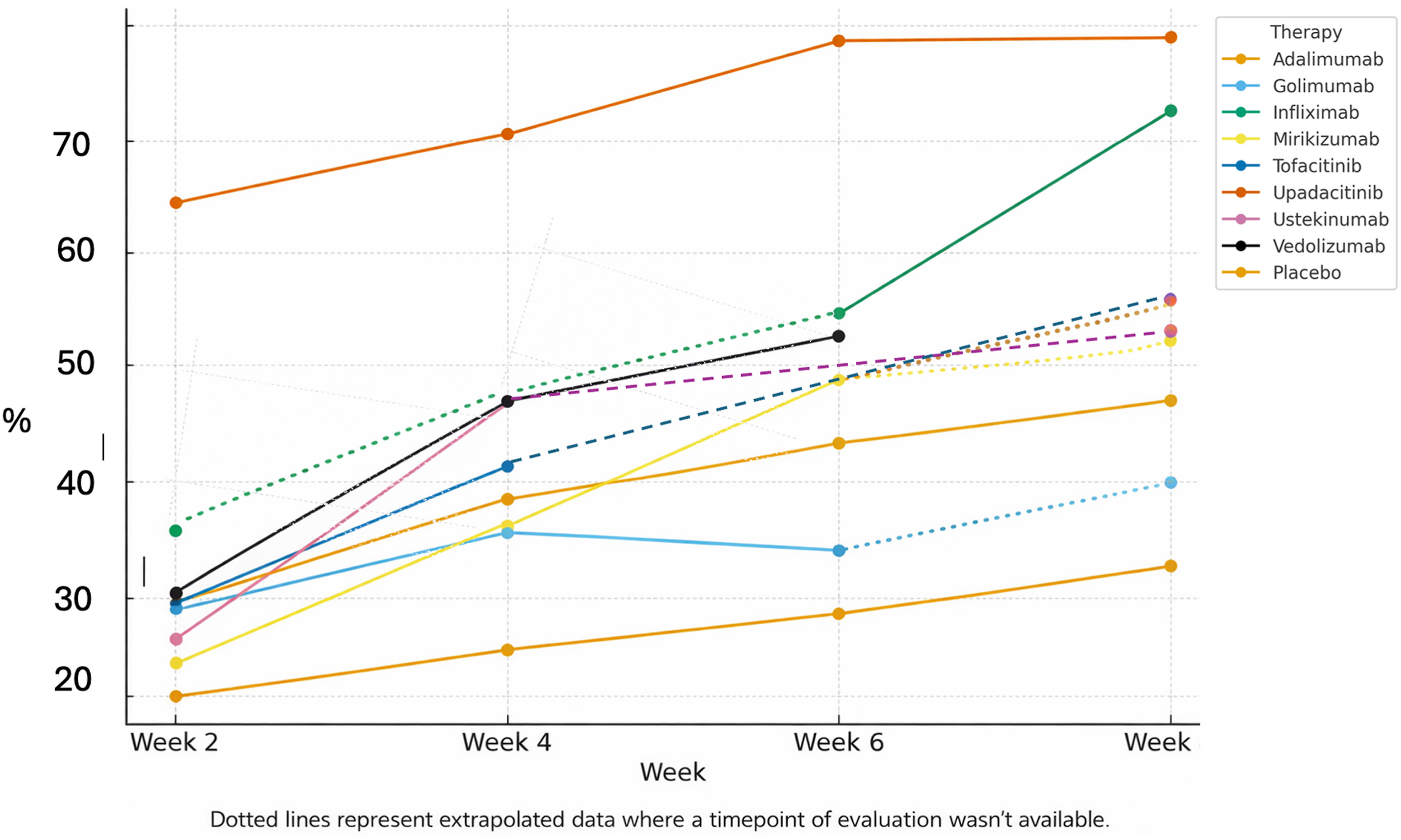
At week 2, upadacitinib had the highest PRO-2 response rate, at 65.0%, followed by infliximab at 36.5%. Response rates for the other active therapies ranged from 24.9% with mirikizumab to 31.1% with vedolizumab, compared with 20.4% with placebo.
In adjusted analyses, upadacitinib was the only therapy associated with significantly higher odds of week 2 PRO-2 response compared with infliximab (adjusted odds ratio, 3.57; 95% CI, 2.40–6.20).
By the end of induction, upadacitinib and infliximab continued to show the highest PRO-2 response rates, at 79.0% and 72.6%, respectively. Upadacitinib showed no significant difference from infliximab in adjusted analyses at postinduction, whereas the other active therapies had significantly lower odds of response.
Clinical relevance: matching therapy to urgency
The study’s clinical relevance, according to the authors, lies in matching treatment choice to the urgency of symptom control. For patients with severe symptoms or near-term hospitalization risk, rapid-onset options may be especially important. For more stable patients, the authors noted that therapies with more gradual onset may still be appropriate when safety profile, route of administration, convenience, or patient preference weigh more heavily.
“Clinicians can use this data to tailor treatment directly to how urgent a patient’s situation is,” Dr. Narula said. “If a patient is suffering severely and we need to keep them out of the hospital right now, upadacitinib or infliximab are the go-to options; if their disease is more stable, we can comfortably opt for therapies with a more gradual onset but perhaps a different safety or convenience profile.”
Response and remission diverged
Remission findings were less straightforward. At week 2, infliximab had the highest PRO-2 remission rate, at 34.9%, while upadacitinib, despite having the highest early response rate, had a week 2 remission rate of 19.7% and lower odds of remission compared with infliximab.
The investigators suggested this may reflect rapid symptom reduction across a broad group of patients who had not yet reached the stricter remission threshold within 14 days. By week 8, ustekinumab and infliximab had the highest unadjusted PRO-2 remission rates, at 53.9% and 51.9%, respectively, although adjusted analyses showed no significant difference between ustekinumab and infliximab.
Limitations and next steps
The analysis had several limitations. Although the investigators harmonized endpoints across trials and adjusted for baseline covariates, the included trials differed in design, induction duration, and assessment timing. Residual confounding remains possible, and the findings may not fully generalize to patients treated in routine clinical practice. The study also focused on biologic-naive patients, so the results may not apply to patients with prior advanced therapy exposure.
“Moving forward, we really need prospective, real-world studies to see if these speed-of-onset differences directly translate into other meaningful IBD-related outcomes, such as fewer hospitalizations and less corticosteroid use,” Dr. Narula said.
Dr. Narula holds a McMaster University AFP Clinician Researcher Award and has received honoraria from Janssen, AbbVie, Takeda, Pfizer, Sandoz, Novartis, Iterative Health, Innomar Strategies, Fresenius Kabi, Amgen, Organon, Eli Lilly, and Ferring.