Gastroenterologists and hepatologists should play a bigger role in treating obesity by making weight-management therapies a routine part of patient care, according to an updated POWER (Practice Guide on Obesity and Weight Management, Education, and Resources) framework. The revised guidance reflects major advances since the original recommendations were released in 2017, including the growing use of anti-obesity medications, endoscopic procedures, bariatric surgery, and coordinated multidisciplinary care.

“Now more than ever, GLP-1–based therapies are playing a central role in obesity management and are shaping broader conversations across healthcare,” first author Andres J. Acosta, MD, PhD, of the Division of Gastroenterology and Hepatology in the Department of Internal Medicine at Mayo Clinic, Rochester, Minn., said in an interview with GI & Hepatology News. “We felt it was important to provide gastroenterologists with an updated review of the field and place these developments in the context of the rapidly evolving obesity treatment landscape.”
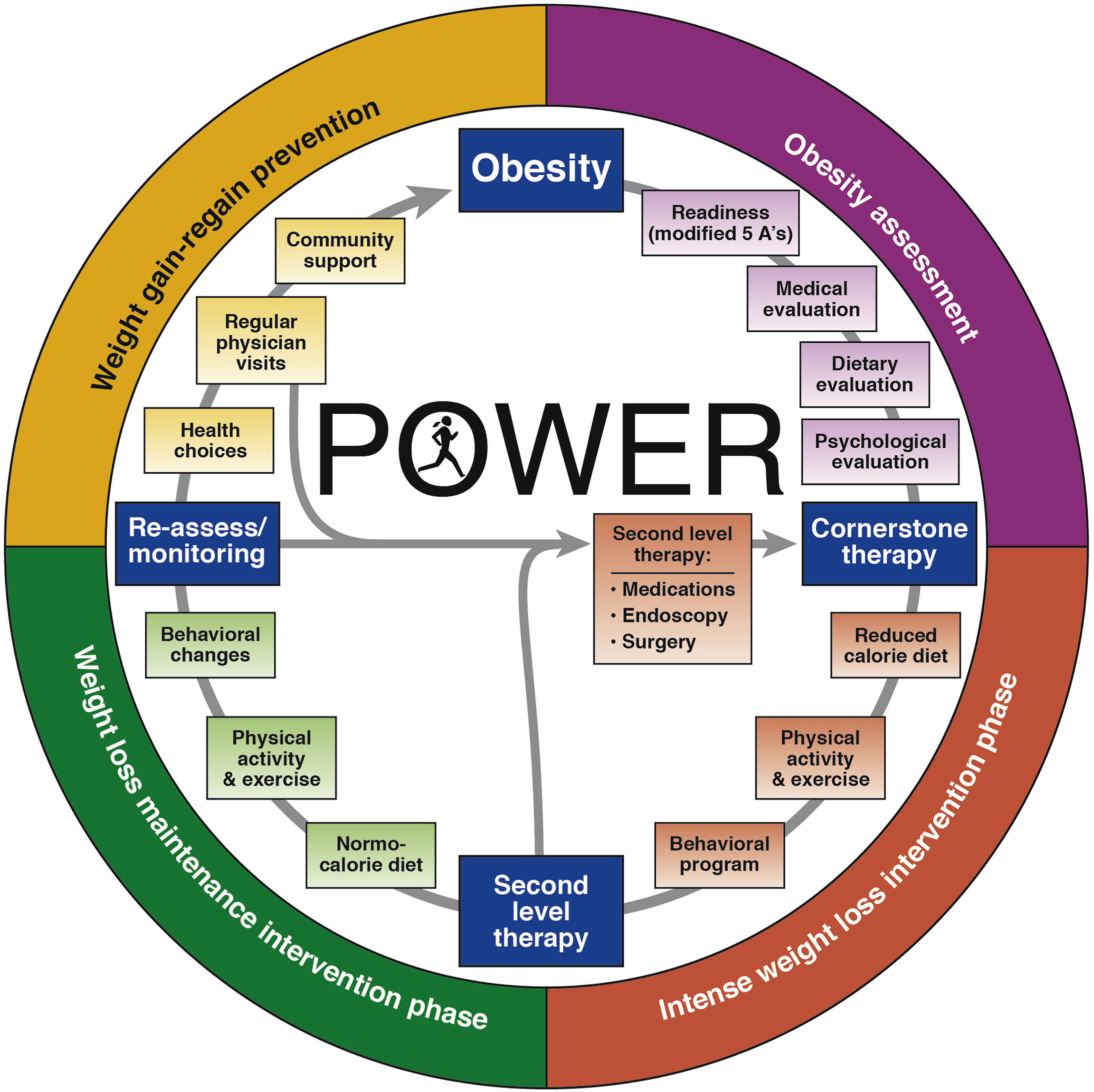
In the commentary, “Revisiting POWER in the GLP-1 Age,” published in Gastroenterology, Dr. Acosta and seven other experts examined the advances that have transformed obesity care over the past several years. These include the rise of glucagon-like peptide-1 (GLP-1) receptor agonists, growing evidence supporting endoscopic bariatric and metabolic therapies, expanded eligibility for bariatric surgery, new insights into the genetics of obesity, and the emergence of value-based care models. The authors emphasized that obesity should be recognized and treated as a chronic, relapsing disease driven by multiple factors, requiring individualized, long-term care.
The update also reflects changing views on how obesity is defined and diagnosed. The authors highlighted recent recommendations that move beyond relying on body mass index (BMI) alone, calling for additional measures such as waist circumference or body fat assessment to confirm excess body fat. They also noted growing recognition that obesity is part of a broader spectrum of cardiometabolic disease, with implications that extend beyond weight alone.
For gastroenterologists and hepatologists, the case for becoming more involved in obesity care is increasingly clear. Patients with obesity often have related gastrointestinal and liver conditions, including gastroesophageal reflux disease, metabolic dysfunction-associated steatotic liver disease (MASLD), gallbladder disease, colorectal neoplasia, inflammatory bowel disease, irritable bowel syndrome, and changes in the gut microbiome. The authors also noted that specialists are seeing more patients who are taking obesity medications or have undergone bariatric procedures.
The framework continues to emphasize lifestyle changes as the foundation of obesity treatment but notes that diet, exercise, and behavioral strategies alone are often not enough to achieve or maintain meaningful weight loss. The authors highlighted evidence supporting multidisciplinary care teams that include physicians, dietitians, behavioral health specialists, and peer-support programs. In one community-based program built on the POWER model, 65% of participants lost more than 10% of their total body weight within a year.
A major focus of the update is the growing role of GLP-1 receptor agonists in obesity treatment. The authors noted that current guidelines recommend adding these medications to lifestyle interventions for appropriate patients. Clinical trials have shown that GLP-1 therapies can consistently produce weight loss exceeding 10% of total body weight, a level associated with improvements in obesity-related conditions such as type 2 diabetes, hypertension, obstructive sleep apnea, and MASLD.
“These medications are targeting the gut-brain axis, and their side effects are GI-related,” Dr. Acosta said. “So, we need to be able to understand these medications, understand obesity, and embrace [our role] in caring for these patients, because they need our help.”
At the same time, the authors highlighted ongoing challenges with the use of GLP-1 receptor agonists, including high costs, limited access, side effects, and difficulty maintaining long-term treatment. In a large database study cited in the review, 65% of patients with obesity stopped GLP-1 therapy within 12 months, compared with 47% of patients with type 2 diabetes and 34% of those with both obesity and diabetes. Discontinuing treatment has been linked to weight regain and the return of metabolic abnormalities.
The commentary also reviewed evidence supporting endoscopic bariatric and metabolic therapies. One of the most established procedures is endoscopic sleeve gastroplasty, which gained Food and Drug Administration recognition as a treatment for obesity after the multicenter randomized MERIT trial. In the study, which included 209 patients, those who underwent endoscopic sleeve gastroplasty achieved 14% total body weight loss at 52 weeks, compared with 1% in the control group. More than 80% of the weight lost was maintained through 24 months, and serious adverse events were reported in 2% of patients. Separate long-term studies found that patients maintained an average total body weight loss of nearly 16% at five years.
Intragastric balloons remain another treatment option, particularly for patients who need a bridge to more definitive obesity therapies. Studies have reported total body weight loss ranging from 7% to 15% at 12 months. In one trial, an adjustable intragastric balloon system produced 15% total body weight loss at 32 weeks, compared with 3% among patients in the control group.
The authors reiterated that bariatric surgery remains the most effective and durable treatment option for many patients with obesity. Current guidelines recommend surgery for patients with a body mass index (BMI) above 35 regardless of obesity-related conditions, as well as for selected patients with type 2 diabetes at lower BMI levels. Typical total body weight loss ranges from 25% to 30% after sleeve gastrectomy, 30% to 35% after Roux-en-Y gastric bypass, and about 40% after duodenal switch. The commentary also cited a systematic review showing that patients who underwent bariatric surgery had a 38% lower risk of death over five years compared with those who did not undergo surgery.
The authors also highlighted growing evidence supporting combination approaches to obesity treatment. In one study, patients who underwent endoscopic sleeve gastroplasty and received liraglutide achieved 25% total body weight loss at 12 months, outperforming results seen with endoscopic therapy alone.
For practicing clinicians, the central message is that obesity care increasingly requires a stepped, personalized approach that matches therapies to patient characteristics, treatment response, and long-term goals.
“Gastroenterologists are on the front lines of obesity, and we should embrace it either to manage as a primary disease or as an adjunct to other diseases that we're managing,” Dr. Acosta emphasized. “The sooner we embrace it, the better we’ll do for our patients.”
Dr. Acosta and multiple coauthors disclosed consulting relationships, speaking activities, research funding, or industry affiliations. Others reported no conflicts of interest.