In a large real-world study of more than 5,000 patients in the Veterans Health Administration system, vitamin D supplementation was linked to fewer inflammatory bowel disease–related emergency department visits, hospitalizations, and corticosteroid prescriptions. The findings suggest that vitamin D may be a simple, low-cost addition to standard IBD care.
“We already knew vitamin D deficiency was bad for IBD patients,” first author Jared A. Sninsky, MD, a gastroenterologist at Baylor College of Medicine and the Michael E. DeBakey VA Medical Center, Houston, told GI & Hepatology News. “The real question was whether supplementing changes outcomes. Studying over 5,000 Veterans with IBD across two decades, we found it does: a 53% relative reduction in hospitalizations and 34% reduction in ER visits. What also sets this apart is that we used multiple quasi-experimental methods to strengthen the causal argument, which most prior observational work hasn’t done.”
Although vitamin D deficiency is common in people with IBD and has been associated with worse disease outcomes, evidence supporting vitamin D supplementation as a treatment strategy has been limited, he added. As a result, current guidelines do not recommend specific vitamin D targets for disease control.
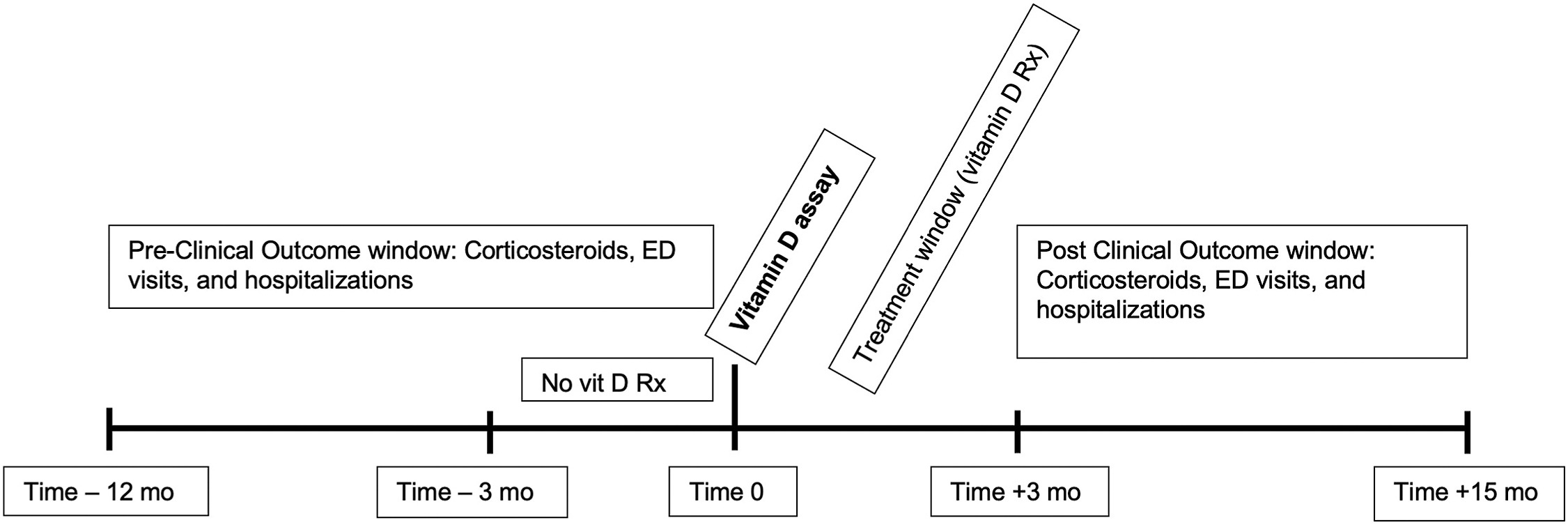
The retrospective study, published in Clinical Gastroenterology and Hepatology, followed 5,021 patients with inflammatory bowel disease (IBD) treated between 2000 and 2023. To determine whether vitamin D supplementation affected clinical outcomes, Dr. Sninsky and colleagues compared changes over time in patients who received supplements with those who did not after vitamin D testing. They used several statistical methods to strengthen their findings, including a difference-in-differences analysis, regression discontinuity, and inverse probability weighting.
The cohort had a median age of 63 years and was mostly male (89%). Ulcerative colitis was the most common diagnosis (58%), followed by Crohn’s disease (39%) and indeterminate colitis (3%). Patients had a median baseline vitamin D level of 23 ng/mL, and 41% received a vitamin D prescription within 3 months of testing.
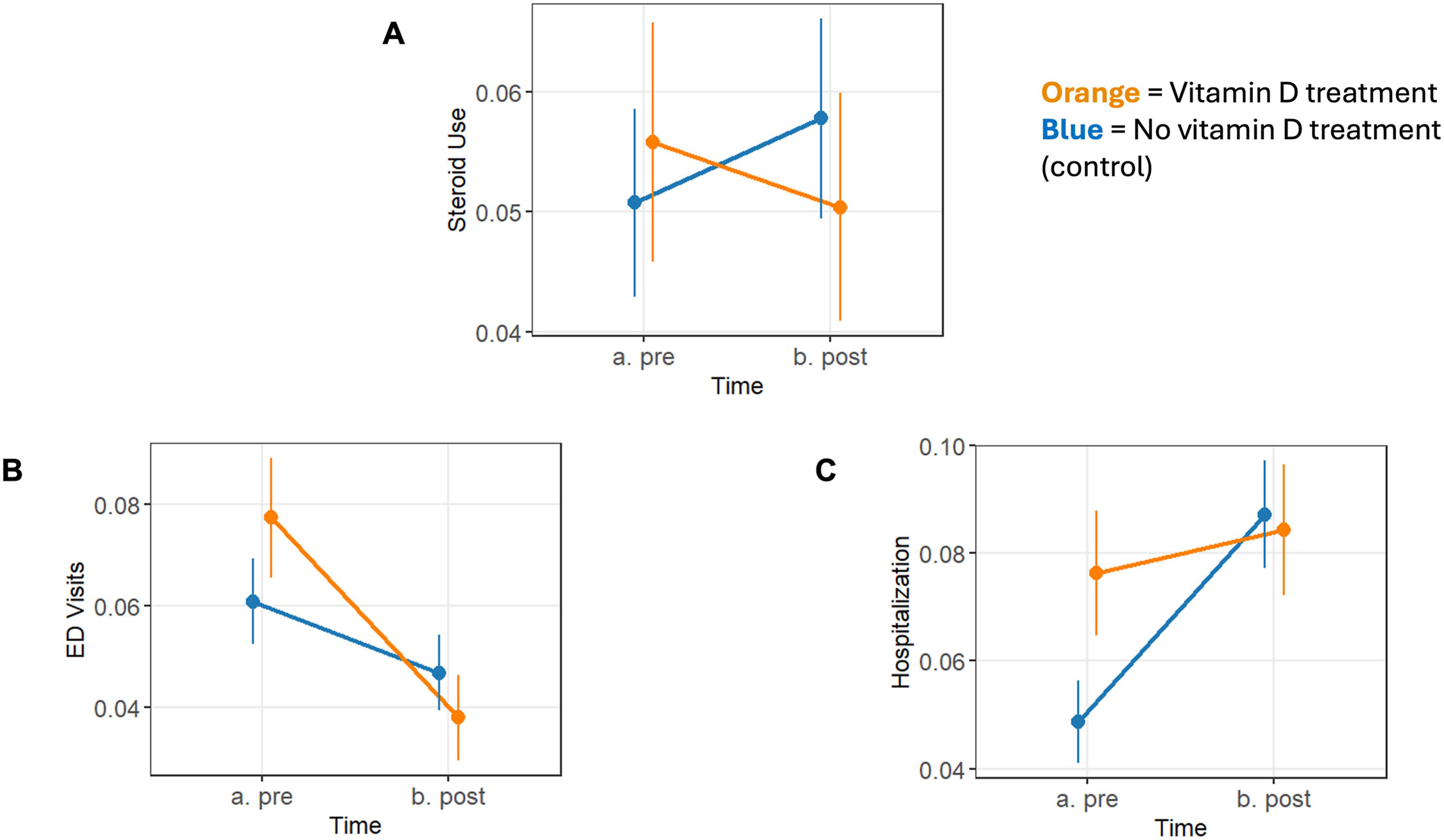
The researchers tracked three measures of disease activity: corticosteroid prescriptions, IBD-related emergency department visits, and IBD-related hospitalizations. They compared rates during the year before vitamin D testing with rates during the year after a three-month post-testing period.
In adjusted analyses, vitamin D supplementation was linked to fewer IBD-related emergency department visits, hospitalizations, and corticosteroid prescriptions. Compared with patients who were not supplemented, those who received vitamin D had 34% fewer emergency department visits, 53% fewer hospitalizations, and 25% fewer corticosteroid prescriptions.
Results differed by disease type. In patients with Crohn’s disease, vitamin D supplementation was associated with fewer emergency department visits and hospitalizations, but not fewer corticosteroid prescriptions. In patients with ulcerative colitis, supplementation was linked to reductions in all three measures of disease activity.
The findings remained consistent across additional statistical analyses. In the inverse probability weighted analysis, vitamin D supplementation was associated with 20% lower odds of corticosteroid use, 25% lower odds of emergency department visits, and 10% lower odds of hospitalization. A separate regression discontinuity analysis, based on the clinical treatment threshold of 30 ng/mL, also found a reduction in corticosteroid use among patients who received supplementation.
Vitamin D levels rose after treatment, though the increase was modest. Median levels increased by just 0.9 ng/mL in patients who were not supplemented, compared with 6 ng/mL in those taking 1,000 IU daily and 8 ng/mL in those taking more than 2,000 IU per day.
The findings suggest that treating vitamin D deficiency may offer benefits beyond bone health in patients with IBD. Supplementation was associated with fewer emergency department visits, hospitalizations, and corticosteroid prescriptions, although the observational nature of the study means a cause-and-effect relationship cannot be confirmed.
The study had several limitations. Most participants were older male veterans, which may limit the generalizability of the findings. About half of treated patients received a relatively low vitamin D dose of 1,000 IU daily, and the study could not account for over-the-counter supplement use. Because the study was retrospective, it also could not identify the optimal vitamin D dose or blood level needed to achieve potential immune-related benefits.
Still, the consistent results across several analytic methods strengthen the signal that vitamin D supplementation may be linked to better clinical outcomes in patients with IBD.
“Our findings demonstrate that vitamin D supplementation reduced the need for IBD-related ED visits and hospitalizations and corticosteroid prescriptions, all surrogates for IBD flares,” the authors concluded. “These results are consistent with previous small-scale randomized trials, reinforcing the role of vitamin D as a low-cost adjunctive therapy in IBD management.”
Funding was provided by the Department of Veterans Affairs Health Services Research and Development Service, the Patient-Centered Outcomes Research Institute, the VA Center for Innovations in Quality, Effectiveness and Safety, and the National Center for Advancing Translational Sciences of the National Institutes of Health. Senior author Jason K. Hou, MD, reported research funding from RedHill Biopharma, Janssen, AbbVie, Celgene, Genentech, Bristol Myers Squibb, Eli Lilly, Lycera, and Pfizer. The remaining authors reported no conflicts of interest.

Expert Insight
GI & Hepatology News invited first author Jared A. Sninsky, MD, a gastroenterologist at Baylor College of Medicine and the Michael E. DeBakey VA Medical Center, Houston, to elaborate on the study results.
How might the findings influence clinical practice?
Dr. Sninsky: I’d hope it pushes clinicians to not just document a low vitamin D level and move on, but to actually treat it. Current guidelines don’t make specific recommendations on vitamin D targets in IBD, which leaves a lot of room for inaction. Our data suggest supplementation is associated with fewer flares, fewer ER visits, and fewer hospitalizations. It’s inexpensive and well-tolerated, so while not replacing biologic therapy, it has real potential as a low-cost adjunct.
What gaps remain, and what research should be done next?
Dr. Sninsky: Optimal dosing is the biggest open question. A large portion of our patients were on 1,000 IU, which is on the lower end, and we need prospective studies to nail down the right dose and target serum level. Our VA population also skews older and male, so broader studies are needed to confirm generalizability. Ultimately, a well-designed RCT with standardized dosing and hard clinical endpoints would really cement vitamin D’s role in IBD care.
Anything else you’d like to add?
Dr. Sninsky: What I’m most proud of is the methodology. Observational IBD research has always struggled with confounding by indication, and by layering three complementary quasi-experimental approaches, we were able to make a stronger causal argument than most real-world studies can. The findings held up across all three methods, which gives me real confidence in the results. I hope it also shows what’s possible with large administrative datasets when you ask the right questions the right way.