A multicenter randomized trial published in Clinical Gastroenterology and Hepatology has found that combining upadacitinib with vedolizumab for eight weeks led to significantly higher rates of endoscopic and clinical remission in patients with moderate-to-severe ulcerative colitis (UC) than vedolizumab alone.
The study explored whether using two advanced therapies together at the start of treatment could improve induction outcomes. Despite the growing number of treatment options for UC, many patients fail to achieve endoscopic remission during induction therapy, prompting continued interest in more effective approaches.
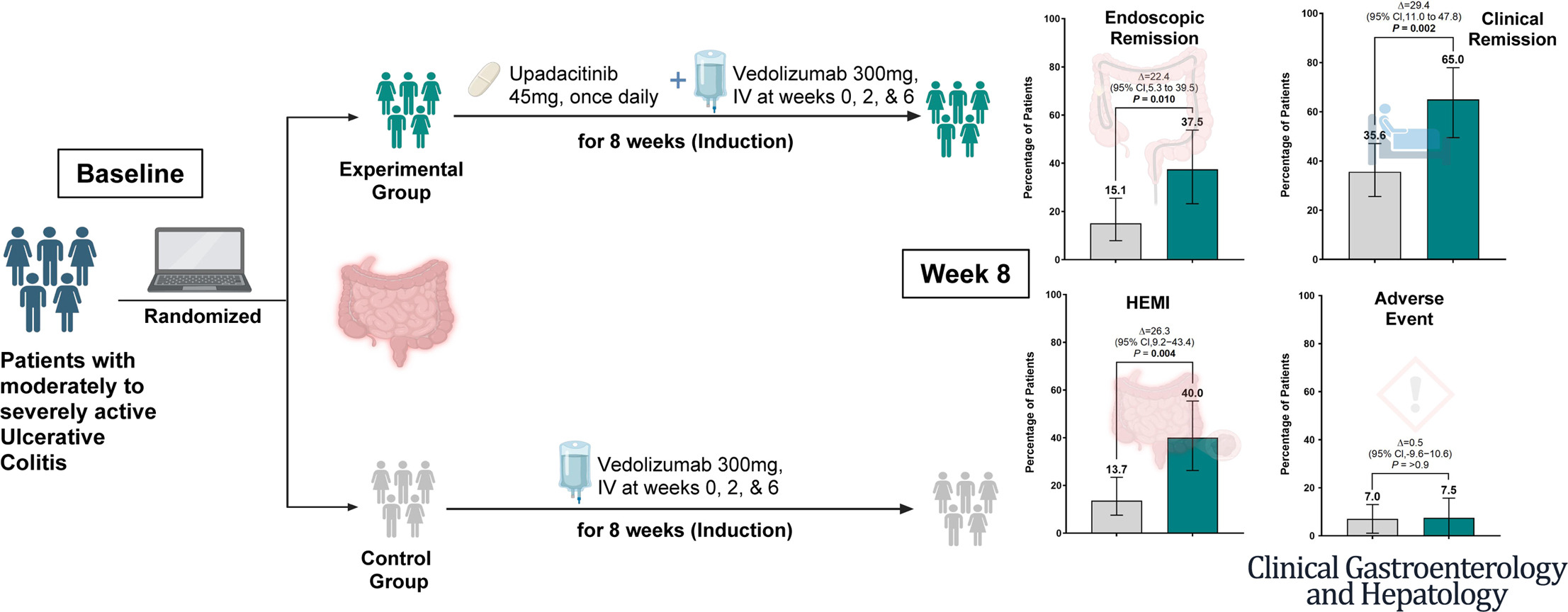
Researchers enrolled 113 adults with moderate-to-severe UC across eight centers in China. Participants received either vedolizumab alone or vedolizumab combined with upadacitinib for eight weeks. The primary endpoint was endoscopic remission, defined as complete resolution of visible inflammation on colonoscopy.
At week eight, endoscopic remission was achieved by 37.5% of patients receiving combination therapy compared with 15.1% of those receiving vedolizumab alone. Clinical remission rates were also higher in the combination arm (65% vs. 35.6%), as were rates of histologic-endoscopic mucosal improvement.
According to study authors, the findings suggest that adding upadacitinib may help patients achieve deeper remission earlier in the treatment course. Both endoscopic healing and histologic improvement are increasingly recognized as important treatment targets because of their association with improved long-term outcomes.
Safety outcomes were similar between the two groups during the eight-week induction period. Adverse events occurred in fewer than 10% of patients in either arm, and no serious adverse events were reported. One patient receiving combination therapy discontinued treatment because of severe rash and elevated lipid levels.
“The primary takeaway is that combining upadacitinib and vedolizumab for an 8eight-week induction period is highly effective for patients with moderate-to-severe ulcerative colitis,” said Jiayin Yao, Aassociate cChief pPhysician and corresponding author. “Our trial demonstrated that this combination more than doubled the rate of endoscopic remission compared to vedolizumab monotherapy. It also significantly increased clinical remission rates and histologic-endoscopic mucosal improvement. Importantly, this enhanced efficacy did not come at the cost of short-term safety; adverse event rates were low and comparable between both groups, with no serious adverse events reported during the 8eight-week period.”
“Historically, advanced monotherapies for UC have faced a therapeutic ceiling, with remission rates rarely exceeding 30%,” Yao said. “Our findings offer a compelling hit-hard-and-early strategy to break through this ceiling. By pairing a potent, rapid-acting small molecule, upadacitinib, with a gut-selective biologic known for its excellent long-term safety, vedolizumab, we can rapidly induce deep mucosal healing. Because early mucosal healing is associated with a drastic reduction in the long-term risk of colectomy, this combination induction approach provides a promising pathway to optimize early patient outcomes while setting the stage for safe, long-term maintenance therapy.”
Several limitations should be considered. The trial was stopped early after an interim analysis demonstrated benefit, resulting in a smaller study population than originally planned. The study was also open-label, and there was no upadacitinib-only arm, making it difficult to determine the specific contribution of combination therapy.
Looking ahead, the investigators emphasized the need for longer-term follow-up. “We are currently continuing the 54-week maintenance phase of this trial, which will provide crucial long-term efficacy and safety data,” Yao said. Those findings will help determine whether the benefits observed during induction can be sustained over time and whether the strategy has a role in routine clinical practice.
The authors reported having no disclosures.