A bedside intestinal ultrasound scan (IUS) performed within the first 48 hours of treatment predicted which children with acute severe ulcerative colitis would not respond to corticosteroids more accurately than standard clinical assessment tools, a prospective study found.
The findings, published in Gastroenterology, suggest that a rapid, noninvasive bedside examination could help physicians make earlier treatment decisions in a condition where delays may increase the risk of complications and surgery.
Paolo Lionetti, MD, PhD, of the gastroenterology and nutrition unit at Meyer Children’s Hospital, Florence, Italy, and colleagues enrolled 60 children with acute severe ulcerative colitis who had not previously received biologic therapy. The patients were treated at 10 pediatric inflammatory bowel disease centers across Europe between 2020 and 2024. All had a Pediatric Ulcerative Colitis Activity Index (PUCAI) score of 65 or higher and received intravenous corticosteroids as the initial treatment, in line with current clinical guidelines.
Each patient underwent two IUS examinations: one within 48 hours of starting corticosteroid treatment and a second between days 5 and 7. Researchers assessed several signs of intestinal inflammation, including colon wall thickness, blood flow in the bowel wall, preservation of bowel wall layers, inflammation of nearby tissue, enlarged lymph nodes, and the Milan Ultrasound Score, which combines wall thickness and blood flow measurements. Treating physicians were not informed of the ultrasound results during the study.
Nearly two-thirds of children in the study (39 of 60) did not respond to corticosteroid treatment and needed additional therapy with infliximab. Ten eventually required surgery to remove their colon within eight weeks because their disease could not be controlled with medication.
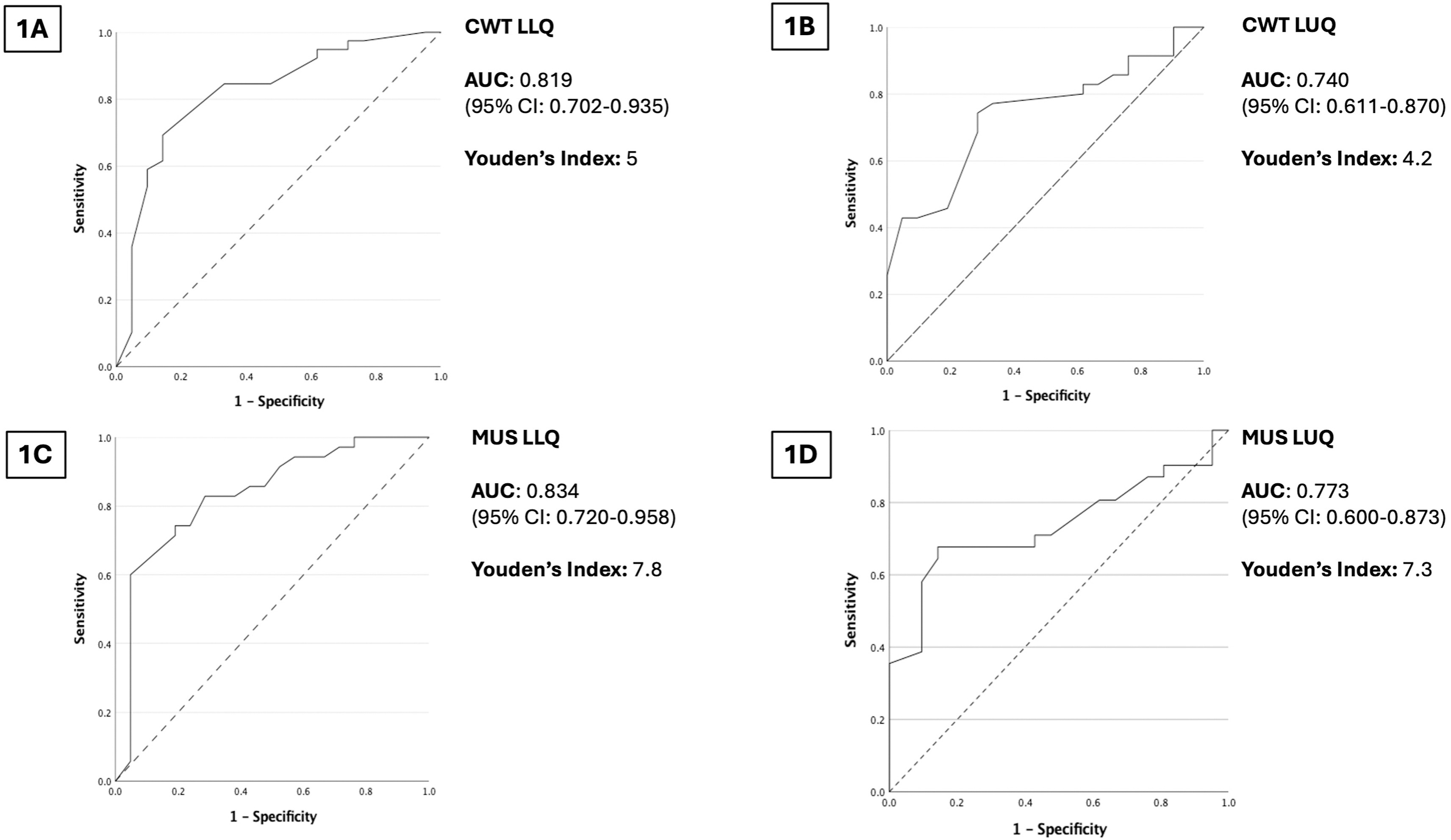
The clearest early predictor of corticosteroid failure on IUS was identified in the left side of the colon. At the first ultrasound exam, children who did not respond to corticosteroids had significantly thicker bowel wall measurements in the left lower quadrant than those who responded, with median measurements of 6 mm compared with 4.2 mm (P < .001). Similar differences were seen in the left upper quadrant. Nonresponders also showed increased blood flow in the bowel wall more often on Doppler ultrasound, a sign of active inflammation.
A bowel wall thickness greater than 5 mm in the lower left quadrant was the best cutoff for predicting corticosteroid failure. Using this threshold, ultrasound correctly identified 85% of patients who did not subsequently respond to steroids and correctly ruled out steroid failure in 67% of those who did respond. The Milan Ultrasound Score performed similarly. A score above 7.8 predicted steroid resistance with 83% sensitivity and 71% specificity.
Notably, both ultrasound measures predicted corticosteroid failure more accurately than the PUCAI score measured at the same time. They also outperformed commonly used blood tests for inflammation, including erythrocyte sedimentation rate and C-reactive protein.
The second ultrasound examination provided another way to identify patients at high risk for poor outcomes. Children who eventually required colectomy continued to show signs of active inflammation on ultrasound, including greater wall thickness, increased vascularity, loss of bowel wall stratification, mesenteritis, and enlarged lymph nodes.
By days five to seven, a left lower quadrant wall thickness greater than 4.8 mm predicted failure of medical treatment with 100% sensitivity. Similarly, a Milan Ultrasound Score above 8.7 identified all patients who ultimately required colectomy or further escalation of treatment. Both ultrasound measures again performed better than the PUCAI score.
The ultrasound findings were also linked to longer-term outcomes. Among patients who did not require colectomy, those who achieved steroid-free clinical remission by eight weeks had significantly reduced left lower quadrant wall thickness and lower Milan Ultrasound Scores on the second ultrasound examination. Lower scores were also associated with the combined outcome of steroid-free remission and fecal calprotectin normalization.
The authors noted several limitations, including the relatively small number of patients, the use of different ultrasound operators and equipment across study sites, and the lack of follow-up beyond eight weeks. Comparisons with endoscopy were also limited because full colonoscopy is generally avoided during episodes of acute severe disease.
Even so, the findings suggest that bedside IUS could play a valuable role during a critical period of treatment, when decisions about escalating therapy can have major consequences for patient outcomes.
“IUS may provide valuable, noninvasive information for early identification of corticosteroid resistance and poor short-term outcomes in pediatric ASUC,” the authors concluded. They also noted that incorporation of colonic wall thickness and Milan Ultrasound Score into routine care pathways “may optimize risk stratification, guide timely escalation of therapy, and support clinical decision-making in this vulnerable population.”
No external funding was received for this study. Several authors reported relationships with pharmaceutical and nutrition companies, including advisory board service, research grants, consulting fees, honoraria, royalties, and speaker fees.
Expert Insight

GI & Hepatology News invited Andrew Day, MB, ChB, MD, Cure Kids Chair of Pediatric Research, University of Otago Christchurch, New Zealand, and Conjoint Professor at the University of New South Wales, Sydney, Australia, to comment on the implications of this work.
What new insights does this study provide?
Dr. Day: This work is important as it adds to the developing data on the role of IUS in ulcerative colitis, especially in ASUC. IUS has become increasingly recognized as a useful tool in the evaluation of the current status of people with IBD. IUS has particular advantages of being non-invasive and being undertaken at the point of care, with immediate results enabling direct feedback to the patient.
This work indicates that IUS, when employed with clear structure, can assist in the prediction of the response to the initial intervention and to the disease course overall.
While the development and broad application of the PUCAI tool has led to more standardized approaches to the management of ASUC, with early consideration of second-line therapies if the response to corticosteroids is inadequate, ASUC remains a concerning event with potential adverse outcomes. This report supports the additive value of IUS in the early assessment of the early disease course in these children.
How might the findings influence clinical practice?
Dr. Day: More units have access to IUS and more practitioners are training in the use of IUS: however, the access to and use of IUS is not universal. The findings of this work could influence clinical practice in the following ways:
More people developing an interest in the use of IUS and undergoing training;
More units (institutions) recognizing the value of IUS and supporting the resources to ensure its availability;
Further studies that confirm and extend the findings of this work, with larger cohorts.
What are the remaining research needs?
Dr. Day: The sample size of the cohort was relatively small, especially in consideration of subgroup analyses. Consequently, extending these evaluations to larger groups and to cohorts of children in further geographical areas would be important. The current cohort included children with various background features (e.g. some with existing disease/some at first presentation; some with oral corticosteroid exposure; some without full endoscopic assessment prior to assessment). While these differences indicate that the group were relatively more severe, they also do raise potential bias.
Further, the study design incorporated the two time points of IUS assessment. This limited the value for some children who needed escalation between the first and second IUS. Further evaluation should consider baseline IUS (at admission/prior to commencing intravenous steroids) and daily repeat assessments.
The results of this work do raise the prospect of the incorporation of IUS into management protocols, potentially in combination with other tools, such as PUCAI, and potentially with biological markers such as calprotectin or other inflammatory markers.
Dr. Day reported having no relevant disclosures.