Patients with fatty liver disease had higher levels of unstable coronary plaque and were nearly twice as likely to experience a major cardiovascular event. This increased risk remained even after researchers accounted for traditional heart disease risk factors and the severity of coronary artery disease, according to an analysis of the Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) trial.

“This study matters because hepatic steatosis is increasingly common and affects approximately 30-40% of the US population,” the study’s first author, Jan M. Brendel, MD, a postdoctoral research fellow in the Cardiovascular Imaging Research Center at Massachusetts General Hospital, Boston,told GI & Hepatology News. “Cardiovascular disease (CVD) is the leading cause of death among individuals with hepatic steatosis. We found that hepatic steatosis was associated with a higher burden of noncalcified, lipid-rich plaque, the type prone to rupture, and with a roughly 1.7-fold higher risk of major adverse cardiovascular events (MACE), independent of standard clinical risk factors, obesity, and the severity of coronary stenosis. This helps clarify one potential pathway linking fatty liver disease to excess cardiovascular risk.”
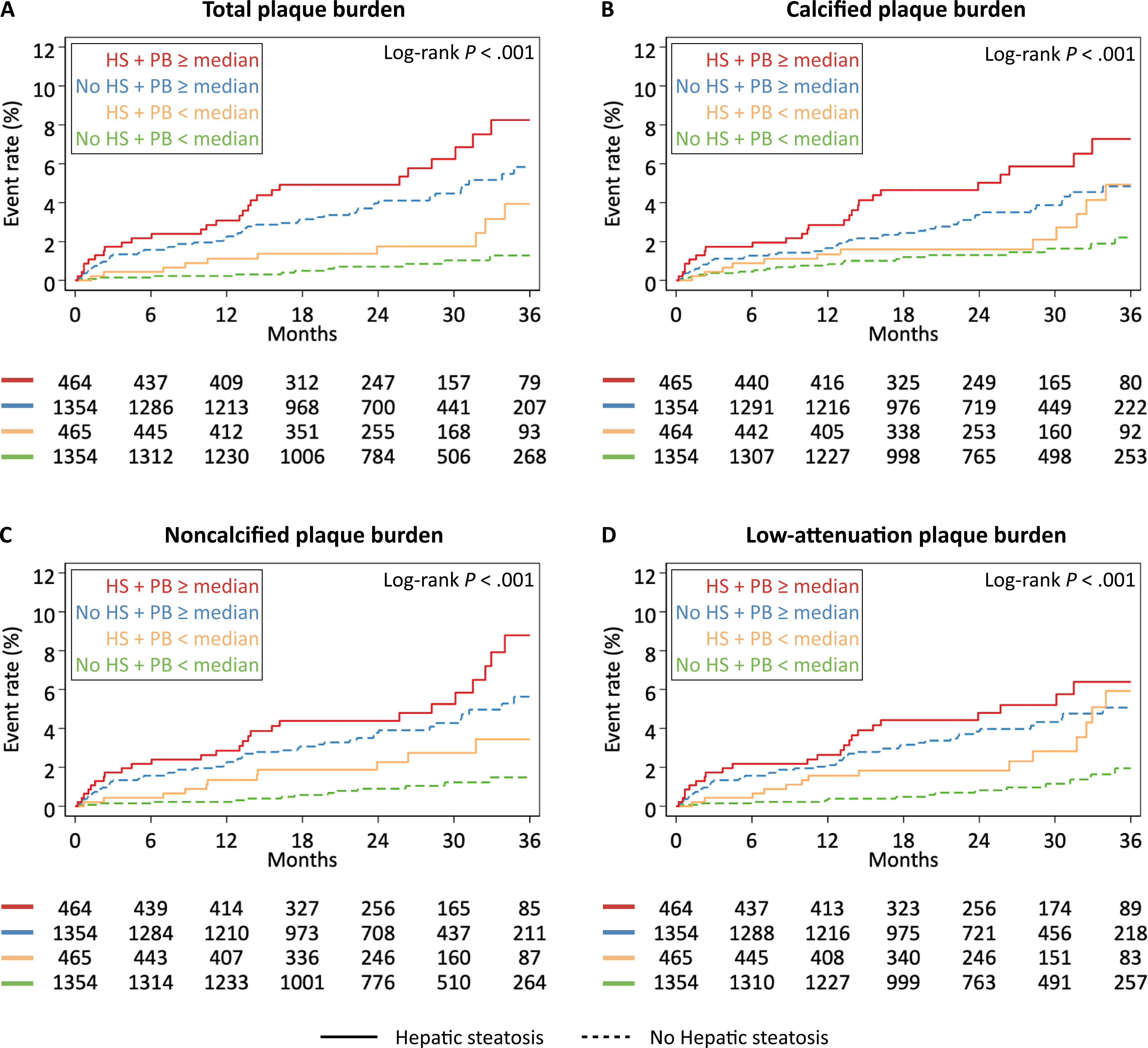
The study, published in Clinical Gastroenterology and Hepatology, included 3,637 patients with stable chest pain who underwent coronary CT angiography in the PROMISE trial. Researchers used CT scans to look for fatty liver disease and analyzed the type and amount of plaque in the coronary arteries. They then tracked patients for a median of 25 months to see whether they experienced a major cardiovascular event, including death from any cause, a heart attack, or hospitalization for unstable angina.
Hepatic steatosis was identified in 929 patients, accounting for 26% of the study population. Compared with patients without steatosis, those with the condition were generally younger, more often male, and more likely to have diabetes, metabolic syndrome, elevated triglyceride levels, and higher levels of inflammatory biomarkers. They also experienced more major adverse cardiovascular events during follow-up, with event rates of 4% compared with 3% among patients without steatosis.
Coronary plaque analysis showed that hepatic steatosis was mainly linked to noncalcified plaque and low-attenuation plaque, both of which can signal more vulnerable atherosclerosis. Patients with steatosis had a median noncalcified plaque burden of 17%, compared with 14% in patients without steatosis. Low-attenuation plaque burden was also higher in patients with steatosis, at 0.08% compared with 0.01%. Although patients with steatosis had greater total plaque volume and higher coronary calcium scores, calcified plaque burden was not significantly different between the groups. Rates of obstructive coronary stenosis were similar.
After adjusting for atherosclerotic cardiovascular disease risk and obesity, hepatic steatosis remained independently associated with a greater plaque burden. Steatosis was linked to a 15% increase in noncalcified plaque burden and a 6% increase in low-attenuation plaque burden. “The risk appears to also live in plaque quality rather than just quantity, which a standard calcium score would miss,” Dr. Brendel noted. Similar results were seen among patients with cardiometabolic risk factors.
The association between hepatic steatosis and cardiovascular outcomes remained significant after adjusting for multiple risk factors. Patients with steatosis had a 69% higher likelihood of experiencing a major adverse cardiovascular event after accounting for cardiovascular risk score, obesity, obstructive coronary stenosis, and noncalcified plaque burden. Among patients with cardiometabolic risk factors, steatosis was associated with a 62% greater likelihood of major adverse cardiovascular events.
To better understand the underlying mechanisms, the investigators conducted mediation analyses to determine whether plaque composition explained part of the link between hepatic steatosis and cardiovascular risk. Noncalcified plaque burden accounted for about 11% of the association between steatosis and major adverse cardiovascular events. Total plaque burden showed a similar pattern, but the finding was not statistically significant. “So, plaque is part of the story but far from all of it, and other pathways are clearly at work,” Dr. Brendel said.
For practicing gastroenterologists and hepatologists, he continued, the findings reinforce that a diagnosis of hepatic steatosis should prompt active cardiovascular risk assessment, not just hepatic follow-up, and ideally coordination with primary care or cardiology. “It's also a reminder that a low or zero calcium score can be falsely reassuring in these patients, because their risk is carried by noncalcified plaque that calcium scoring doesn't capture,” Dr. Brendel said. “And because noncalcified plaque is modifiable - it responds, for example, to lipid-lowering medication - there's a real opportunity to identify these patients earlier and treat their cardiometabolic risk more aggressively.”
The researchers noted several limitations of the study, including its observational design, the use of CT imaging rather than liver biopsy to identify hepatic steatosis, the lack of follow-up imaging data, and the absence of information on alcohol use or viral hepatitis. Also, because the study population consisted of patients with chest pain, the findings may not be generalizable to lower-risk populations.
“Our findings support the concept of a liver–coronary axis and raise important questions for future studies, including whether aggressive cardiometabolic prevention can modify noncalcified plaque burden and reduce cardiovascular events in patients with hepatic steatosis,” Dr. Brendel concluded.
The study was supported by grants from the National Heart, Lung, and Blood Institute. Dr. Brendel and some authors reported having no relevant disclosures. Others reported consulting relationships, research funding, employment, advisory roles, or stock interests involving cardiovascular imaging and biotechnology companies, including Cleerly, HeartFlow, Elucid, AstraZeneca, MedImmune, BioMarin, and others.