With respect to serious infections, ustekinumab appears to be the safest advanced therapy for inflammatory bowel disease.
Among advanced therapies for inflammatory bowel disease (IBD), serious infection rates were lowest with ustekinumab, according to data published in Clinical Gastroenterology and Hepatology by lead author Anaïs Bertrand, a master’s student at Université Paris-Saclay in France, and colleagues. Rates were highest with Janus kinase (JAK) inhibitors and intermediate with anti–tumor necrosis factor (TNF) agents and vedolizumab in this large population-based nationwide French cohort.
“In addition, each drug class appears associated with distinct infection profiles,” corresponding author Antoine Meyer, MD, PhD, also of Université Paris-Saclay, told GI & Hepatology News. “Corticosteroids doubled the risk of serious infection.”
Study details
The analysis was based on a nationwide French cohort of patients with IBD aged over 15 years who initiated treatment between 2014 and 2024. Treatments included vedolizumab, ustekinumab, JAK inhibitors, anti-TNF agents, and aminosalicylates. Serious infections were evaluated according to treatment exposure, with propensity score weighting used to account for indication bias.
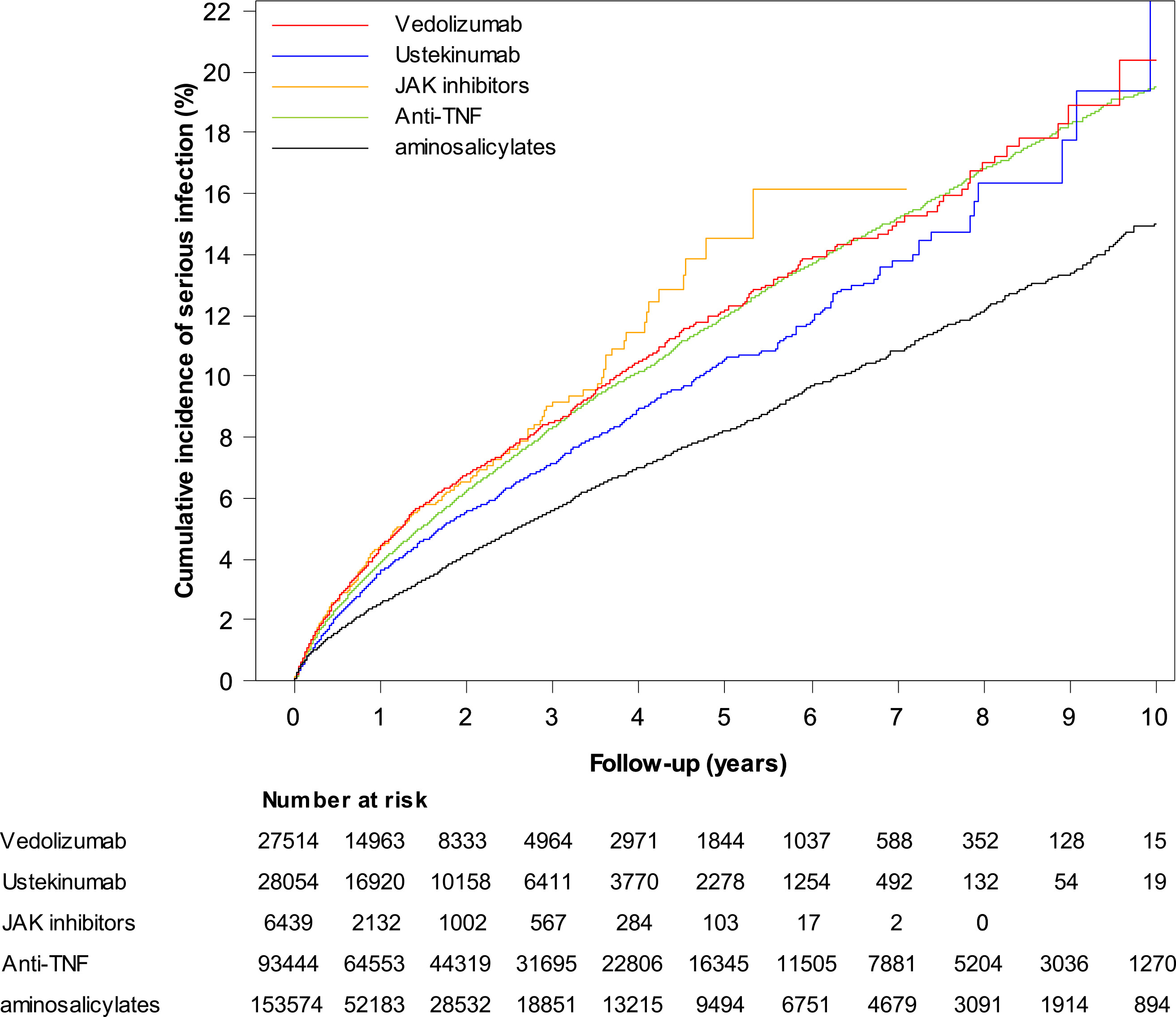
In total, 309,025 treatment initiations were recorded among 219,229 patients, including 27,514 starting vedolizumab, 28,054 ustekinumab, 6,439 JAK inhibitors, 93,444 anti-TNF agents, and 153,574 aminosalicylates. The median patient age was 41 years, 52.0% were women, and 45.3% had Crohn’s disease.
During a median follow-up of 1.0 years, 15,081 serious infection events were identified.
Serious infection risk by treatment
Relative to aminosalicylates, the adjusted hazard ratio (aHR) for serious infection was 1.05 (95% CI, 0.98–1.11) with ustekinumab — not a statistically significant difference — versus 1.29 (95% CI, 1.24–1.34) with anti-TNF agents, 1.38 (95% CI, 1.30–1.46) with vedolizumab, and 1.63 (95% CI, 1.45–1.84) with JAK inhibitors. Compared with anti-TNF agents, the aHR was 0.81 (95% CI, 0.76–0.86) with ustekinumab and 1.27 (95% CI, 1.12–1.43) with JAK inhibitors. The aHR for vedolizumab versus anti-TNF agents was 1.07 (95% CI, 1.01–1.13), though the authors noted this difference disappeared in several sensitivity and subgroup analyses. Patterns were consistent across IBD types.
Anti-TNF agents and vedolizumab showed the strongest associations with skin, upper respiratory tract, and central nervous system infections, whereas JAK inhibitors appeared most strongly associated with herpesvirus infections and anti-TNF agents with mycobacterial infections.
The risk of serious infection was increased with concomitant corticosteroids (aHR, 2.06) and thiopurine/methotrexate (aHR, 1.11).
Dr. Meyer concluded, “These findings may help clinicians better individualize treatment decisions according to patients’ infectious risk factors and comorbidities. In particular, corticosteroid exposure remained a major driver of serious infection risk, emphasizing the importance of minimizing steroid use whenever possible.”
Because this was an observational study using nationwide administrative health care data, residual confounding cannot be excluded, according to Dr. Meyer. The follow-up duration was also shorter for newer therapies, including JAK inhibitors.
Future research should focus on long-term safety outcomes — such as malignancy, cardiovascular events, and thromboembolic complications — as well as comparative safety differences among individual JAK inhibitors, Dr. Meyer said. Additionally, the authors noted that further work will be needed in the coming years once sufficient real-world data become available for newer agents, including anti–interleukin-23 therapies and sphingosine-1-phosphate inhibitors.
Co-authors Aurélien Amiot and Franck Carbonnel reported consulting, lecture, and advisory board fees from multiple pharmaceutical companies including AbbVie, Janssen, Pfizer, and Takeda; co-author Antoine Martin reported board and lecture fees from AbbVie and Janssen. Lead author Bertrand and corresponding author Dr. Meyer reported no conflicts of interest.