Long-term treatment with dupilumab was associated with sustained clinical, endoscopic, and histologic remission in pediatric and adult patients with eosinophilic esophagitis (EoE), according to results from the retrospective multicenter DUPEOETALY study published in Clinical Gastroenterology and Hepatology.
The observational study evaluated 167 patients with confirmed EoE treated at 50 Italian pediatric and adult gastroenterology, allergy, and clinical immunology centers between 2023 and 2024. According to the study, patients received dupilumab through compassionate-use or off-label programs before regulatory approval for EoE in Italy.
The median age at dupilumab initiation was 21.5 years, and 77.8% of patients were male. Investigators reported that 76% of patients had a personal history of atopy. Before treatment with dupilumab, 94% of patients had received proton pump inhibitors, and 86.2% had received topical corticosteroids. According to the study, nonresponse rates to proton pump inhibitors and topical corticosteroids were 96.8% and 92.4%, respectively.
Kristle Lynch, MD, of the University of Pennsylvania and a member of the AGA Quality Committee, told GI & Hepatology News that the findings add meaningful real-world context to the existing trial data.
“The DUPEOETALY study provides real-world evidence that long-term dupilumab therapy can achieve sustained and near-complete remission in patients with EoE,” Dr. Lynch said. She noted the cohort included patients who were refractory or intolerant to prior treatments such as proton pump inhibitors and topical corticosteroids.
Investigators assessed symptoms using the dysphagia symptom questionnaire, endoscopic severity using the EoE endoscopic reference score, and histologic activity using peak eosinophil counts per high-power field (eos/HPF). Outcomes were evaluated at baseline and at weeks 12, 24, 36, 48, 60, and 72.
According to the study, all primary outcomes improved significantly over time. The least squares mean dysphagia symptom questionnaire score decreased from 22.14 at baseline to 4.94 at week 12 and 0.21 at week 72 (P < .001). Peak eosinophil counts decreased from a mean of 36.80 eos/HPF at baseline to 2.03 eos/HPF at week 12, reaching −0.64 eos/HPF at week 72 (P < .001). The mean EoE endoscopic reference score decreased from 3.95 at baseline to −0.07 at week 12 (P < .001), which investigators wrote reflected “near-complete endoscopic resolution of inflammation and remodeling features across the population.”
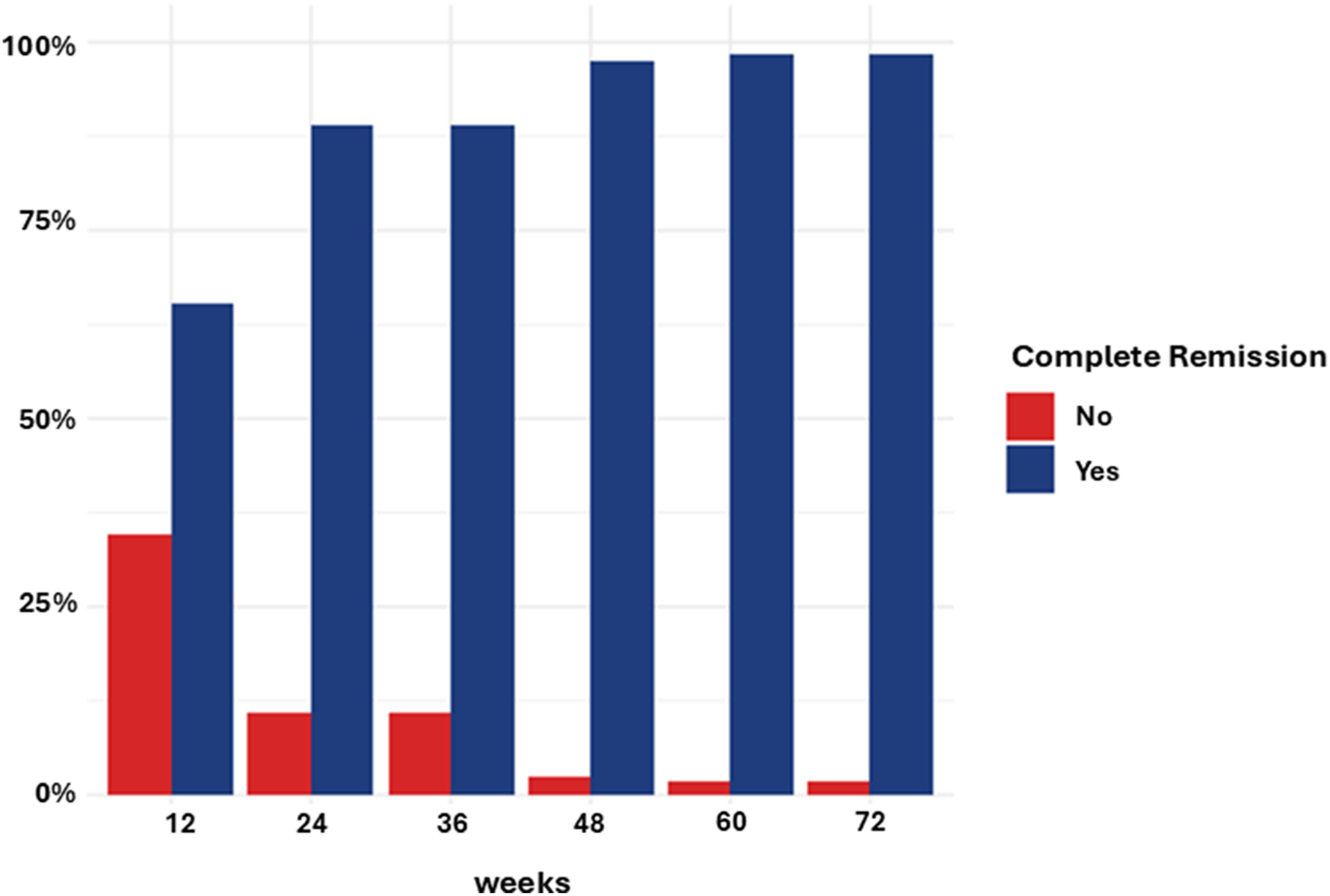
The authors defined complete remission as a dysphagia symptom questionnaire score of five or less, endoscopic reference score of two or less, and fewer than 15 eos/HPF. According to the study, 73% of patients achieved composite remission at week 12, with remission rates exceeding 90% from week 24 onward. By week 72, 98.3% of patients met the study's remission criteria.
The investigators reported that treatment response did not significantly differ according to sex, diagnostic delay, prior esophageal dilation, or personal history of atopy. Baseline eosinophil count also was not significantly associated with treatment response. However, higher baseline dysphagia symptom questionnaire and endoscopic reference scores were associated with lower odds of achieving complete remission at week 12, according to multivariable analysis.
The study included both pediatric and adult patients. According to the authors, adults experienced a longer median diagnostic delay than pediatric patients, with adults having a median delay of four years compared with one year in children. The authors wrote that adults were more likely to have received proton pump inhibitors and undergone esophageal dilation before dupilumab initiation, reflecting “more advanced or complicated disease stages at the time of biologic initiation.”
The authors reported that patients with fibrostenotic features, including esophageal rings, strictures, or prior dilation, were included in the cohort. In the discussion, they noted clinical and endoscopic improvements in patients with fibrostenotic disease during dupilumab treatment.
Safety findings were favorable throughout follow-up. According to the study, six patients (3.8%) experienced adverse events, including three cases of injection-site reactions, two episodes of transient arthralgia, and one case of mild conjunctivitis. No serious adverse events were reported, and no patients discontinued treatment because of intolerance.
Dr. Lynch said patients experienced marked improvements in esophageal symptoms, endoscopic findings, and histologic inflammation at 72 weeks, and she referred to the remission rates, which approached 98%, as “remarkable.”
“No treatment-emergent serious adverse events were noted, and no patients discontinued therapy due to intolerance, reinforcing both the tolerability and durability of dupilumab treatment,” she told GI & Hepatology News.
Dr. Lynch said the findings may affect long-term management strategies for refractory disease.
“For clinicians, the key takeaway is that dupilumab offers a highly effective steroid-sparing targeted therapy capable of improving multiple aspects of EoE simultaneously, in patients refractory to prior therapy,” she said. “These findings may influence patient care by encouraging long-term maintenance treatment strategies and advancing a more personalized approach to EoE management focused on sustained disease remission.”
The authors acknowledged several limitations, including the retrospective study design, the lack of standardized follow-up schedules, and the absence of centralized histologic review. The authors also noted that dupilumab frequently was initiated alongside ongoing therapies, including proton pump inhibitors, topical corticosteroids, or dietary interventions, which may affect interpretation of treatment outcomes.
Dupilumab was provided free of charge through Sanofi's Managed Access Program; Sanofi had no role in study design, data collection, analysis, or reporting but was given the opportunity to review the manuscript before submission. Several authors reported speaker, consultant, or advisory relationships with Sanofi/Regeneron and other pharmaceutical companies; full disclosures are listed in the published study.