The recent US approval of semaglutide for fibrotic metabolic dysfunction-associated steatohepatitis is likely to add relatively few newly eligible patients because most already qualify for treatment through existing indications for obesity or high-risk type 2 diabetes, a population-based analysis found.

“Although candidacy for GLP-1 receptor agonists is high, penetration of use for MASH treatment remains suboptimal,” one of the study authors, Zobair M. Younossi, MD, MPH, professor and chairman of the Global NASH/MASH Council Center for Outcomes Research in Liver Disease, told GI & Hepatology News. “The main challenge in GI is to assure that primary care and diabetology colleagues risk stratify at-risk patients for MASH and start appropriate treatment according to published guidelines.”
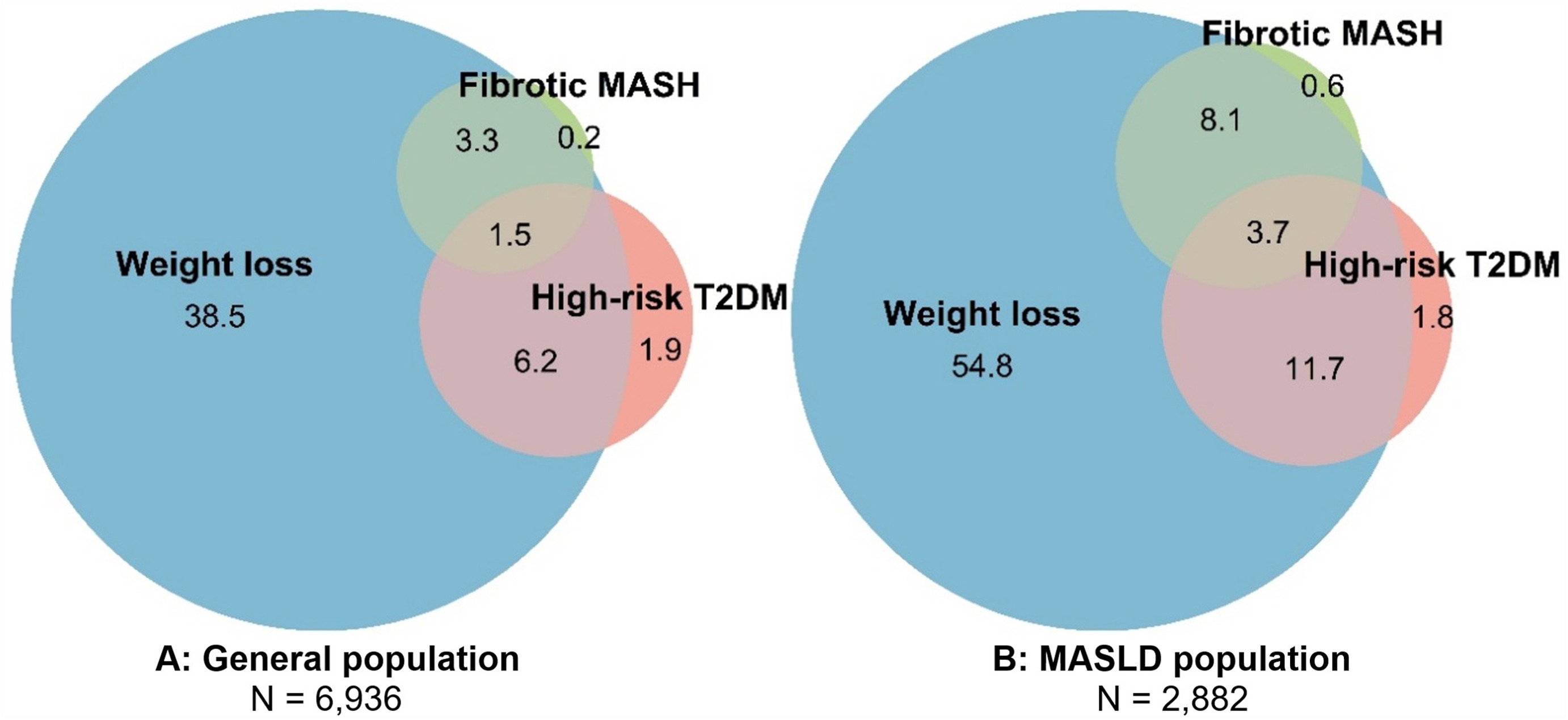
Researchers analyzed data from 6,936 adults in the National Health and Nutrition Examination Survey (NHANES) from 2017 to 2020 and found that 52% of US adults already qualified for semaglutide based on FDA-approved indications for weight loss or high-risk type 2 diabetes. Adding fibrotic metabolic dysfunction-associated steatohepatitis (MASH) as an approved use had little impact on eligibility, increasing the rate by less than 1 percentage point.
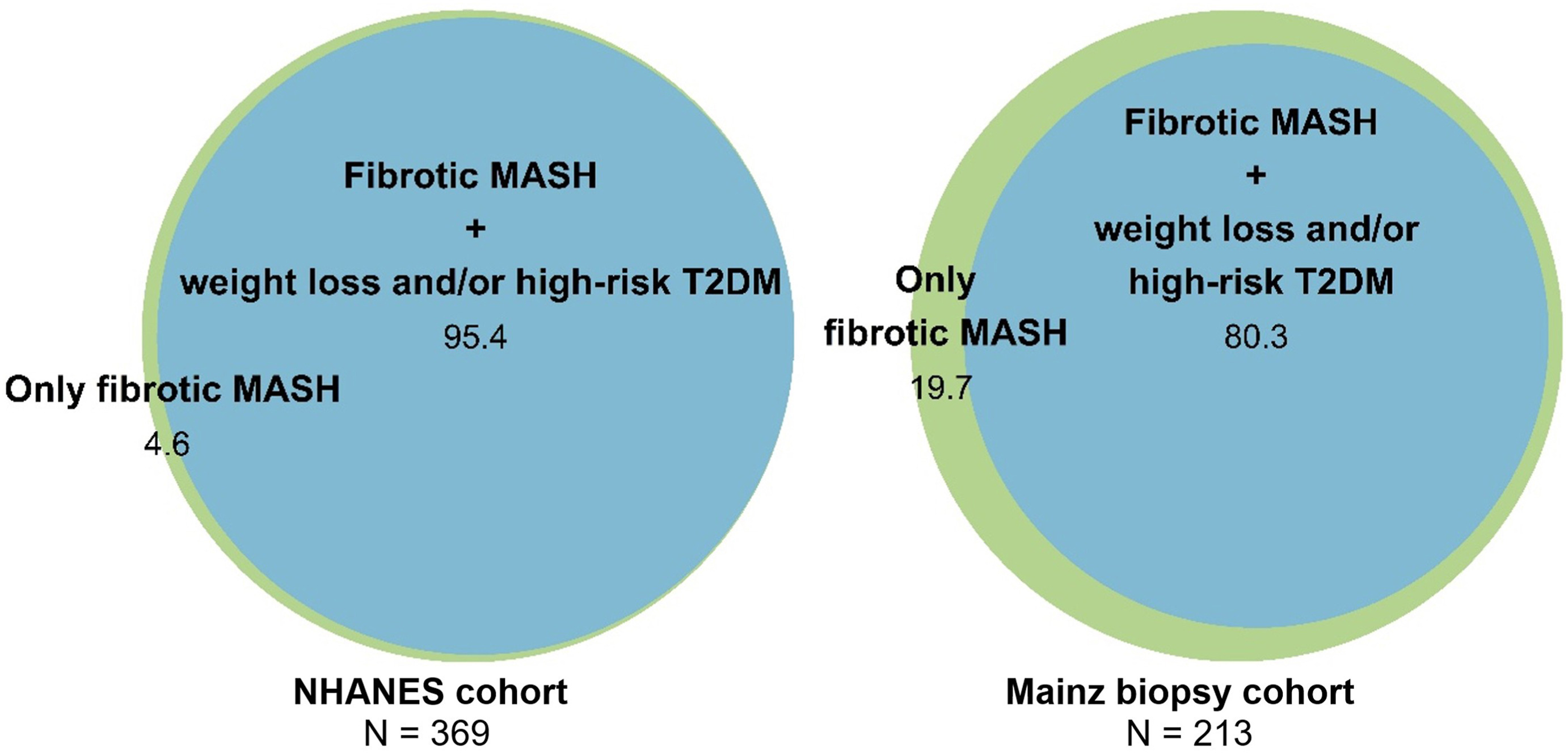
The study, published in Gastro Hep Advances, examined the impact of semaglutide’s newly approved indication for patients with MASH and stage F2-F3 liver fibrosis. Researchers used transient elastography data to identify patients with metabolic dysfunction-associated steatotic liver disease (MASLD) and fibrotic MASH, while excluding those with viral hepatitis or excessive alcohol use. The findings were confirmed in a separate German cohort of 213 patients with biopsy-confirmed MASLD and F2-F3 fibrosis.
Among patients with MASLD, 80% already qualified for semaglutide under existing indications, and adding fibrotic MASH increased eligibility only marginally, to 81%. Among patients with fibrotic MASH, 95% were already eligible because of obesity-related conditions, high-risk type 2 diabetes, or both, while only 5% qualified solely under the new liver disease indication.
The weight-loss indication accounted for most semaglutide eligibility. Among patients who qualified under existing indications, 74% had dyslipidemia, 62% had hypertension, 33% had prediabetes, 17% had obstructive sleep apnea, and 11% had cardiovascular disease. Overall, 41% of adults had MASLD and 5% had fibrotic MASH.
The validation cohort yielded similar results. Among patients with biopsy-confirmed MASLD and F2-F3 fibrosis, 80% already met eligibility criteria for semaglutide through existing indications. Those who qualified only under the new fibrotic MASH indication generally had lower liver stiffness measurements and lower noninvasive fibrosis scores than patients who were already eligible because of obesity- or diabetes-related conditions.
The authors noted that a key limitation of the study is that it was based on US population data and therefore may not be generalizable to countries with lower rates of obesity and metabolic disease. Fibrotic MASH was identified using noninvasive criteria in NHANES rather than liver biopsy, and some cardiovascular risk data were unavailable in the validation cohort. The authors also pointed to ongoing debate over the accuracy and interpretation of liver stiffness measurements in people with obesity.
Dr. Younossi noted that pharmacotherapy “must always be accompanied by lifestyle modification to minimize ultra processed foods, high sugary drinks, and alcohol.”
Funding was provided by the Foundation for Liver and Gastrointestinal Research, Rotterdam, the Netherlands. Multiple authors reported consulting fees, research support, speaker fees, advisory roles, or clinical trial involvement with pharmaceutical companies developing therapies for metabolic liver disease.

Expert Insight
GI & Hepatology News invited Mohamed Elsaid, PhD, MPH, assistant professor in the department of biomedical informatics at The Ohio State University, to share his perspective on the study’s findings. His research focuses on developing strategies to improve the prevention and early detection of gastrointestinal diseases, including liver, colorectal, and pancreatic cancers.
Why is this study important?
Dr. Elsaid: The ESSENCE trial showed that semaglutide improves liver histology in fibrotic MASH, which is why the FDA approved it for that use. For the current analysis, Laurens A. van Kleef, MD, PhD, and colleagues asked the next question, which is the more practical one. Once fibrotic MASH is on the label, how many more patients can actually be treated? In a nationally representative sample of US adults, eligibility moved from 51.5% to 51.8%. That is, in effect, no change at all. The reason is overlap, and that is the real finding of this work. In this study, almost everyone who qualified for semaglutide because of fibrotic MASH already qualified because of obesity or high-risk diabetes. Roughly 95% of the fibrotic MASH group met a conventional indication, primarily due to weight-related conditions. So the study makes visible something we lose track of when we organize care by organ system, which is very important. In metabolic liver disease, the obesity patient, the diabetes patient, and the liver patient are usually one person.
How might the findings influence clinical practice?
Dr. Elsaid: I would read it less as a new reason to prescribe and more as a reason to go looking. If most people with fibrotic MASH are already eligible through their weight or their diabetes, then the patient in the endocrinology or primary care clinic with obesity and type 2 diabetes is very often the same patient with unrecognized liver fibrosis. The useful move is to pick those patients up with simple noninvasive tests, rather than waiting on a separate liver workup to confirm an eligibility that, for most of them, is already there. This brings us to the larger point: we need to stop running these conditions in separate clinics. One drug now sits at the intersection of obesity, diabetes, and liver disease, and care should be built around that fact. We also need to factor in that semaglutide works alongside diet and activity, not instead of them, and access is still far from uniform.
There is also an easy-to-miss effective dosing issue. As per the ESSENCE trial, the dose that benefits the liver is 2.4 mg weekly with 1.7 mg weekly as a fallback if 2.4 mg is not tolerated. This is higher than the dose many patients take for diabetes, sometimes as low as 1.0 mg. A patient who is “already on semaglutide,” in other words, may not be on a MASH-approved dose, even though lower doses may still provide metabolic or liver-related benefit.
Where are the knowledge gaps, and what still needs investigation?
Dr. Elsaid: A few stand out. First is the gap between eligibility and treatment. Knowing that half of US adults qualify says nothing about how many will start the drug, stay on it, and have it covered. That chain, from eligibility to real uptake by insurer, is where the policy questions actually sit, and it is not something this study could measure.
Second, the phenotype is noninvasively modeled, not biopsy-confirmed. In NHANES, fibrotic MASH was inferred from CAP-defined steatosis and a single liver stiffness reading, not from a biopsy. Elastography stages fibrosis reasonably well, but it does not see the inflammation and ballooning that define steatohepatitis. Nonfibrotic factors and test variability can also elevate liver stiffness, so repeat or sequential testing may be needed to reduce misclassification. The number here is best understood as treatment-eligible fibrotic MASLD, and the harder task of defining who truly has at-risk disease, with repeat testing or a two-step pathway, is still in front of us.
Dr. Elsaid disclosed that he receives funding from AstraZeneca.