A telemonitoring program allowed patients with active inflammatory bowel disease (IBD) to shift much of their follow-up out of the clinic without compromising disease control, according to a multicenter randomized trial across Spain published in Clinical Gastroenterology and Hepatology.
The trial randomized 159 adults starting immunosuppressants, biologic therapies, or Janus kinase inhibitors at 24 hospitals to use the Telemonitoring of Crohn's Disease and Ulcerative Colitis (TECCU) app (75 patients) or receive standard care (84 patients), with follow-up over one year. The study was powered to test whether telemonitoring was noninferior to standard care for clinical remission.

“This study is important because the evidence on the economic impact of telemonitoring in inflammatory bowel disease is limited,” study author Javier Del Hoyo, MD, PhD, of the gastroenterology department at La Fe University and Polytechnic Hospital, Valencia, Spain, told GI & Hepatology News. “IBD associates a high consumption of resources, further increased by the rise in its incidence and prevalence around the world. Moreover, early intervention is crucial to improve long-term outcomes, and telemonitoring can provide a flexible follow-up method adapted to the disease evolution in each patient with IBD. However, the efficiency of telemonitoring in terms of cost-effectiveness has been studied in a few centers thus far.”
Participants had either Crohn's disease or ulcerative colitis. The primary endpoint was time spent in remission; researchers also assessed quality-adjusted life years (QALYs), a measure combining quality and length of life, and tracked health care use, travel expenses, lost work productivity, and other out-of-pocket patient costs.
After 52 weeks, patients in the TECCU group spent an average of 30.7 weeks in remission, compared with 34.1 weeks in the standard-care group — a difference that did not reach statistical significance. Among patients with Crohn's disease, time in remission was nearly the same in both groups; among patients with ulcerative colitis, the numerical difference favored standard care, though the authors reported that telemonitoring remained noninferior overall. Blood and stool markers of inflammation, including C-reactive protein and fecal calprotectin, improved similarly in both groups, and quality of life improved in both. EuroQol 5-Dimension 5-Level scores rose from 0.82 to 0.87 in the TECCU group and from 0.76 to 0.89 in the standard-care group.
The clearest difference was in how care was delivered. Patients in both groups had a similar number of scheduled contacts with their care teams — 6.9 per patient with TECCU versus 7.0 with standard care — but telemonitoring shifted those contacts away from the clinic. TECCU patients averaged 3.1 in-person visits versus 4.8 with standard care, and 3.7 remote contacts versus 2.3.
That shift was associated with lower costs. Average health care spending was 370 euros per patient in the TECCU group versus 406 euros with standard care, with most of the difference coming from fewer in-person visits. Patients using TECCU also traveled less for appointments, averaging 69 km during the study versus 175 km with standard care, with correspondingly lower travel expenses (17 vs 39 euros per patient). The authors reported that TECCU participation was associated with savings of about 52 km of travel, 13 hours of work time, and 13 euros in travel-related expenses per patient.
In the cost-utility analysis, telemonitoring was less expensive than standard care in about 74% of simulated scenarios. Using a willingness-to-pay threshold of 20,000 euros per QALY, the authors reported that telemonitoring had a 94% probability of being cost-effective at 12 weeks and a 90% probability at 52 weeks. At 12 weeks, TECCU was associated with an estimated 698 euros in savings per additional week of remission and 998 euros per QALY; at 52 weeks, the corresponding figures were eight euros per week of remission and 1,441 euros per QALY.
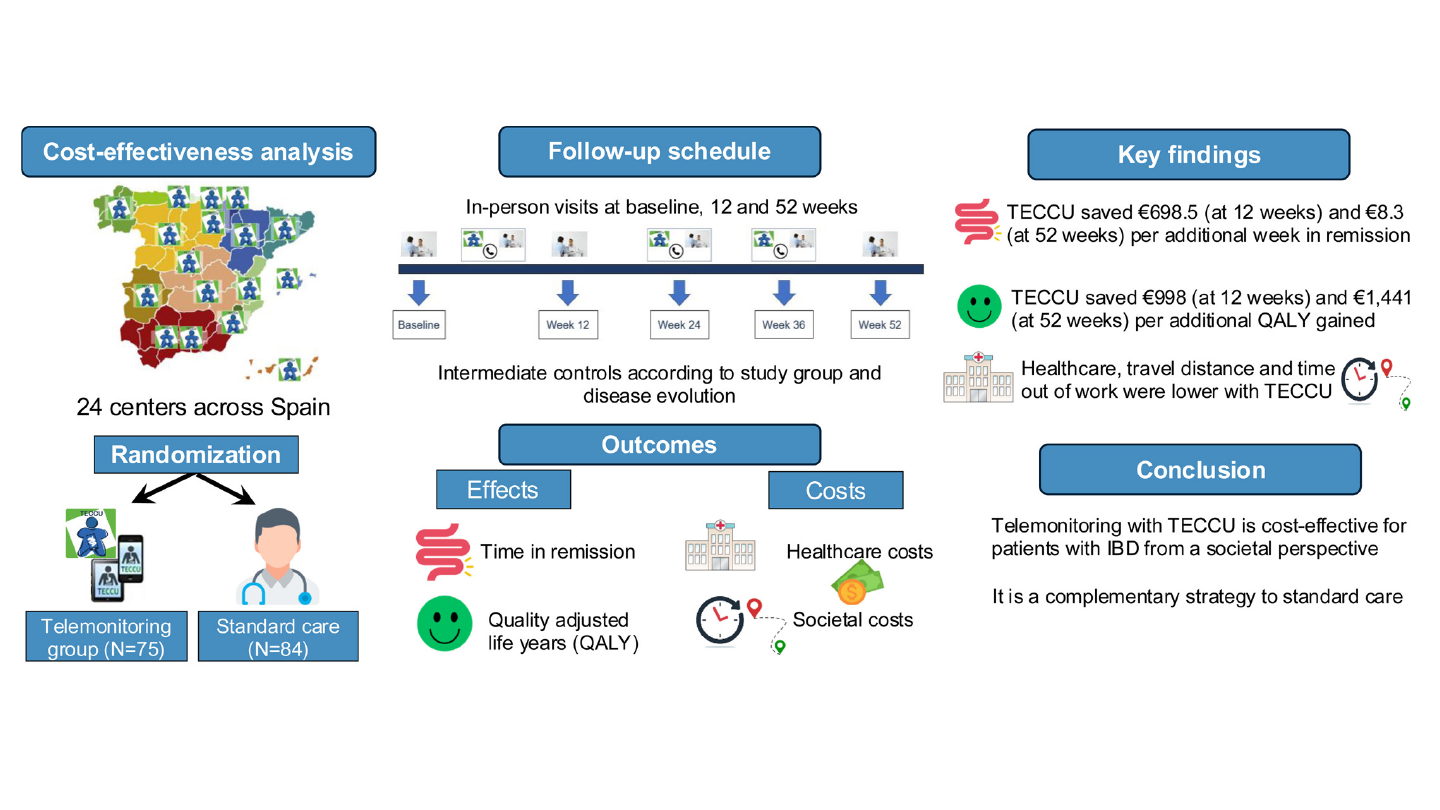
“The results presented in this study can guide decision-makers regarding the implementation of telemonitoring in patients with IBD,” Del Hoyo said. “To date, one of the barriers to the widespread use of telemedicine was the lack of economic data, and our work provides evidence which supports telemonitoring as an efficient alternative in this setting. Therefore, these findings provide a rationale for the adoption of telemonitoring as a complement to standard care in patients with active IBD in daily practice.”
He and his coauthors acknowledged several limitations. The trial was powered to assess noninferiority for clinical remission, not differences in quality of life, productivity, or economic outcomes. Follow-up was limited to 52 weeks, potentially missing longer-term cost trends. The COVID-19 pandemic may also have influenced health care use patterns and increased remote contacts in the standard-care arm.
“This study is the result of more than 10 years of work,” Del Hoyo said. “Now we know that telemonitoring can complement standard follow-up efficiently for both healthcare system and patients. We might consider that cost-estimates are context-dependent, but our study showed that the cost-effectiveness profile of telemonitoring is similarly beneficial in alternative costing scenarios. This reinforces the reproducibility of the results not only in Spain, but also in other healthcare systems.”
The study was funded by the Instituto de Salud Carlos III, co-funded by the European Regional Development Fund, and by an investigator-initiated study from Johnson & Johnson. The authors reported no conflicts of interest related to the study.