Patients who had a positive fecal immunochemical test (FIT) after a colonoscopy and before they were due for their next recommended screening or surveillance examination had a higher risk of post-colonoscopy colorectal cancer (PCCRC) than patients who had no interval FIT or a negative interval FIT, according to a population-based study published in Clinical Gastroenterology and Hepatology.
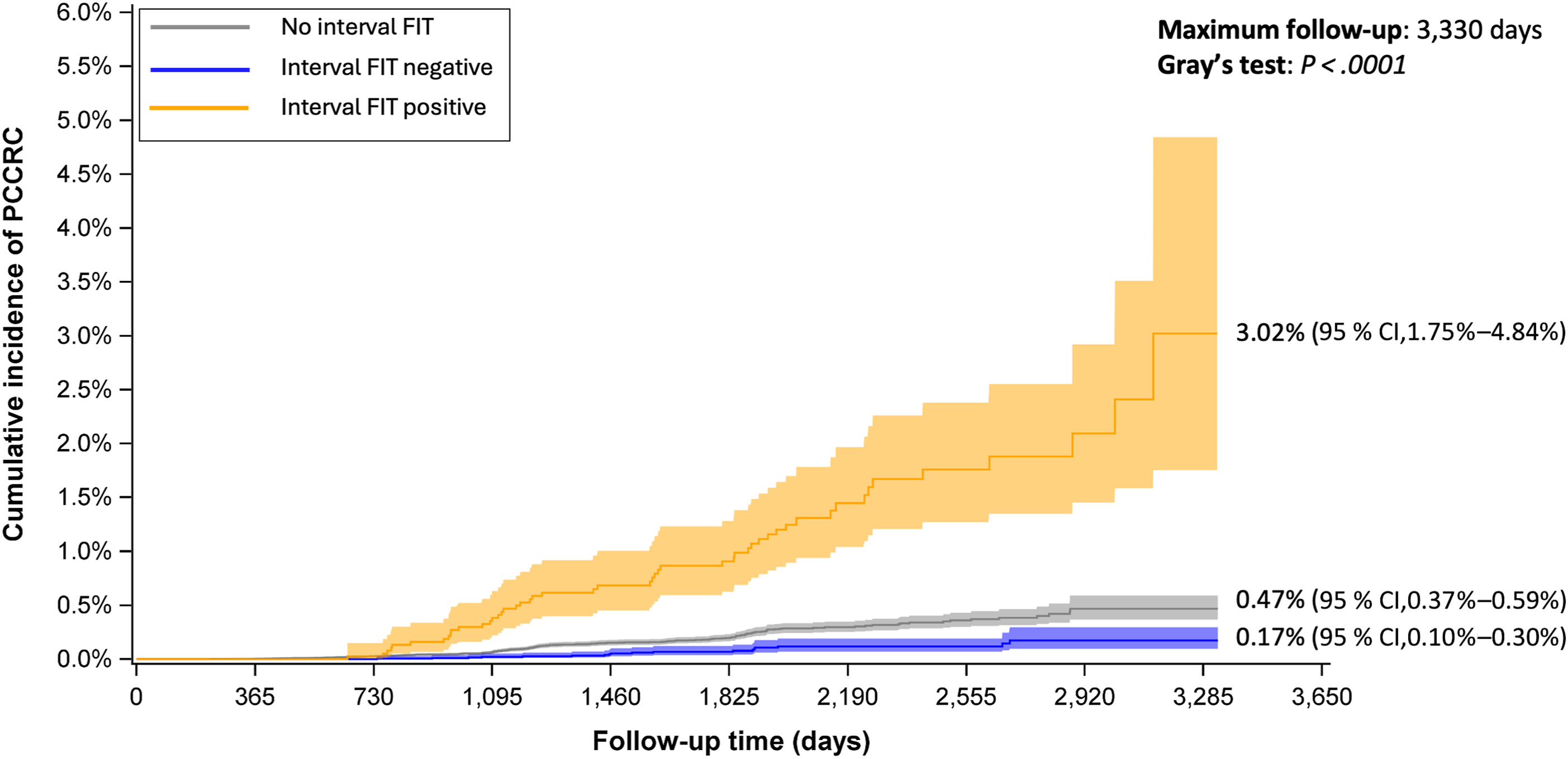
During a median follow-up of approximately 43 months, 275 of 169,117 patients developed PCCRC. The cumulative incidence of PCCRC was 0.47% among patients who did not undergo interval FIT testing, 0.17% among those with a negative interval FIT, and 3.02% among those with a positive interval FIT, according to the study.

“This study demonstrates that patients who have a positive fecal immunochemical test (FIT) after a colonoscopy and before they are next due for colon screening are at higher risk of colorectal cancer when compared to patients who have an interval negative FIT or do not have FIT performed,” lead author Jennifer J. Telford, MD, MPH, FRCPC, CAGF, FACG, told GI & Hepatology News. “The key takeaway is that despite a recent colonoscopy, patients with a positive FIT should be offered repeat colonoscopy.”
The authors wrote that the optimal management of patients with an unplanned positive FIT after colonoscopy remains uncertain. Although U.S. and European guidelines suggest considering repeat colonoscopy in this setting, those recommendations have been based on limited evidence.
To evaluate the association between interval FIT results and PCCRC risk, investigators conducted a retrospective cohort study using data from the British Columbia Colon Screening Program. The analysis included 169,117 patients who underwent colonoscopy between 2013 and 2021. Patients with incomplete colonoscopy, inflammatory bowel disease, or a personal history of colorectal cancer were excluded.
The primary outcome was PCCRC, defined as colorectal cancer diagnosed more than six months after the index colonoscopy and before the end of the recommended screening or surveillance interval. Among study participants, about 15% completed a FIT after colonoscopy but before they were due for repeat screening or surveillance. Most of those tests were negative, while a smaller proportion were positive.
After adjustment for demographic characteristics, family history, prior colonoscopy history, colonoscopy findings and other factors, patients with a positive interval FIT remained at significantly increased risk of PCCRC compared with patients who did not undergo interval FIT testing. By contrast, a negative interval FIT was associated with a lower risk.
“Patients with a positive interval FIT are at increased risk of PCCRC and should be offered repeat colonoscopy,” the authors concluded.
The association remained consistent across multiple sensitivity analyses. Investigators also accounted for differences in follow-up time and variation among physicians performing colonoscopy.
According to the authors, patients with a positive interval FIT who underwent an additional colonoscopy before a PCCRC diagnosis continued to have an elevated risk compared with patients who did not undergo interval FIT testing, although the risk was lower than that observed in the overall interval FIT-positive group. “The risk of PCCRC was reduced, but still significant, for patients in the interval FIT positive group who had an additional colonoscopy between their index colonoscopy and PCCRC diagnosis,” the authors wrote.
The study was conducted within an organized screening program that does not recommend routine interval FIT testing for patients already enrolled in colonoscopy surveillance or for those not yet due for repeat screening. However, interval FIT testing still occurred in a subset of patients, allowing investigators to evaluate outcomes associated with positive and negative test results.
The authors identified several strengths of the study, including its large sample size, population-based design, detailed colonoscopy data and linkage with a provincial cancer registry. They wrote that these features improved the accuracy of risk estimates and minimized the risk of missing cancer diagnoses.
The authors acknowledged that the study's retrospective design limited the ability to account for all factors associated with colorectal cancer risk. In addition, the indication for interval FIT testing was unknown. According to the authors, some FITs may have been ordered because patients lacked a regular primary care provider, while others may have been used to investigate symptoms. The authors also noted that the findings should be interpreted in the context of local screening practices, including FIT positivity thresholds and underlying colorectal cancer prevalence.
The authors reported having no disclosures.