In a nationwide Swedish study, patients with isolated ulcerative proctitis were not more likely to develop rectal cancer or high-grade rectal dysplasia than people in the general population. The study followed nearly 16,000 patients for a median of more than 10 years.
The findings, published in Gastroenterology, support current European and US guideline recommendations that patients with limited ulcerative colitis (UC) disease extent can follow standard population colorectal cancer (CRC) screening practices rather than intensive inflammatory bowel disease (IBD) surveillance programs.

“Previous research has shown that patients with isolated ulcerative proctitis do not have an increased risk of CRC,” lead study author Åsa H. Everhov, MD, PhD, of the Department of Surgery at Stockholm South General Hospital, Sweden, told GI & Hepatology News. “However, the incidence of rectal cancer has not been evaluated separately.”
Researchers analyzed data from several Swedish national health registers, including the Swedish Inflammatory Bowel Disease Quality Register, National Patient Register, Cancer Register, and Cause of Death Register, to identify incident cases of isolated ulcerative proctitis diagnosed between 1997 and 2023. The investigators compared 15,957 patients with ulcerative proctitis against 158,079 matched population comparators without IBD, CRC, or colectomy.
Patients and comparators were matched by sex, age, and residence. Inclusion required two UC records in the National Patient Register or one such record in combination with entry in the quality register documenting proctitis as the initial disease extent. Patients with prior CRC or proctocolectomy were excluded.
The median age at diagnosis was 38 years, and 56% of patients were women. A family history of CRC was reported in 7% of patients with ulcerative proctitis and 6% of comparators.
During follow-up, inflammation stayed limited to the rectum in 60% of patients. In the remaining 40%, the disease spread farther into the colon: 23% developed left-sided colitis and 17% developed extensive colitis.
By the end of follow-up, 16% of patients had received azathioprine, 13% had been treated with advanced therapies, 3% underwent colectomy, and 1% underwent proctocolectomy.
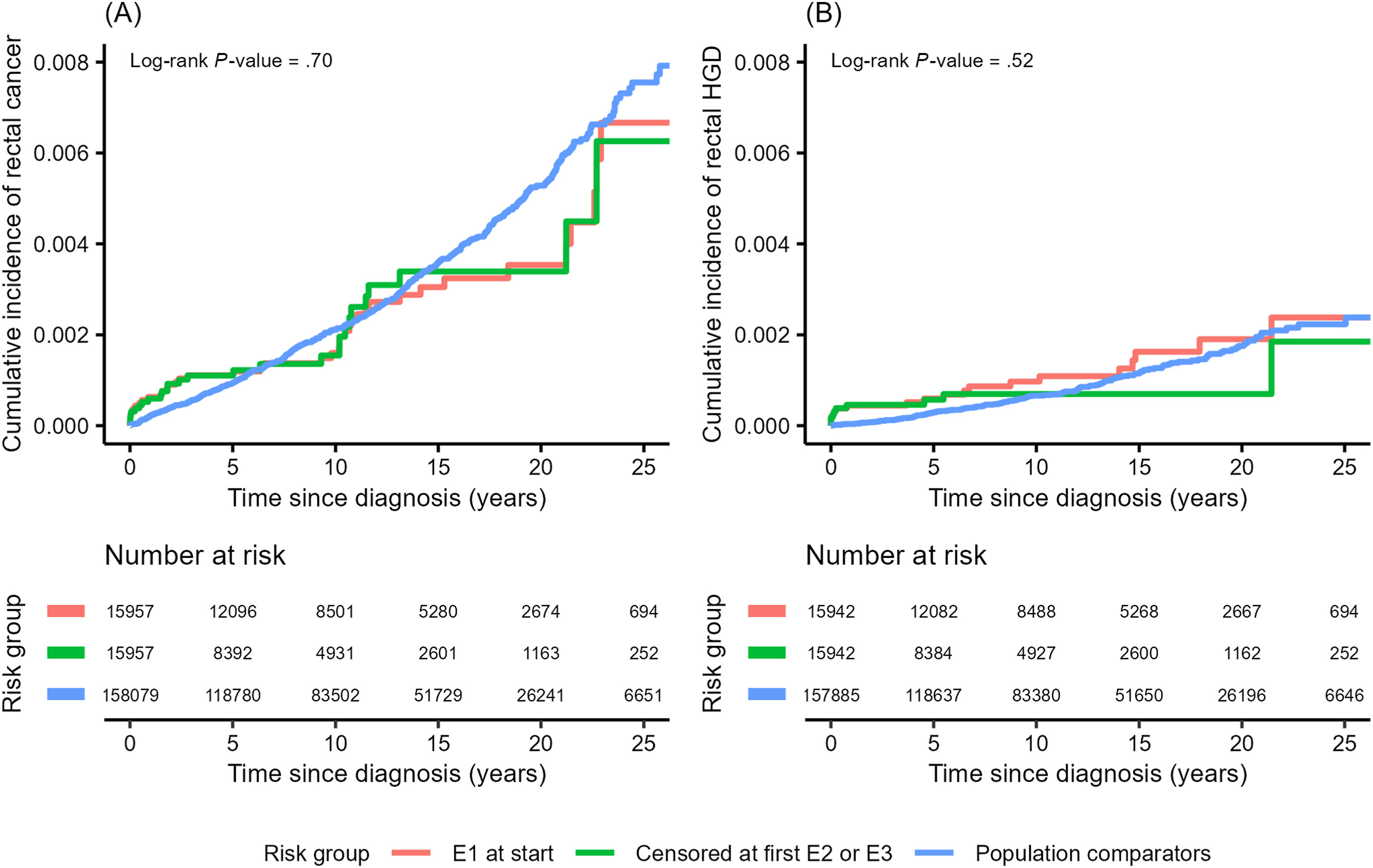
Although chronic rectal inflammation has long been thought to increase cancer risk, the overall rates of rectal cancer were nearly the same in both groups. At five years, rectal cancer incidence was 0.11% among patients with ulcerative proctitis compared with 0.09% in matched comparators. At 10 years, incidence was 0.16% in patients and 0.21% in comparators.
Standardized rectal cancer incidence rates were 31 per 100,000 person-years among patients with ulcerative proctitis and 33 per 100,000 person-years among comparators. When investigators censored patients at the time of disease extension beyond the rectum, incidence rates remained identical at 33 per 100,000 person-years in both groups.
Rates of high-grade rectal dysplasia were also similar between the groups. After five years, the cumulative incidence was 0.06% in patients with ulcerative proctitis versus 0.03% in the comparison group. At 10 years, rates increased slightly to 0.10% and 0.07%, respectively.
In the primary analysis, standardized incidence rates for high-grade dysplasia were 15 cases per 100,000 person-years in patients with ulcerative proctitis and 11 cases per 100,000 person-years in the comparison group. Results were similar even after accounting for disease extension.
“The findings can influence clinical practice by supporting individualized approach to cancer surveillance in IBD,” Dr. Everhov said. “Current surveillance strategies are influenced by the known elevated cancer risk in extensive UC. This study confirms that patients with disease confined to the rectum do not require cancer surveillance beyond that of the general population. That can help reduce unnecessary colonoscopies, lower health care burden, and provide reassurance to patients.”
She and her coauthors noted several limitations of the study, including its reliance on International Classification of Diseases (ICD) coding, which may have led to some misclassification. They also pointed out the possibility of detection bias, since ulcerative proctitis and rectal cancer can cause similar symptoms.
However, a sensitivity analysis excluding the first year of follow-up did not change the results. Additional analyses limited to patients with disease extension documented in the IBD quality register also produced findings consistent with the primary analysis.
The authors said unmeasured confounding factors, including smoking habits, diet, and participation in cancer screening, could not be excluded but were unlikely to meaningfully alter the conclusions.
The study was funded by the Swedish Research Council, Swedish Cancer Society, Swedish Medical Association, Bengt Ihre Research Fund, and the Regional Agreement on Medical Training and Clinical Research between Stockholm County Council and Karolinska Institutet. Several authors reported relationships with pharmaceutical companies including Janssen, Pfizer, AbbVie, Takeda, Ferring, Bristol Myers Squibb, MSD, Galapagos, Alfasigma, Baxter, Ethicon, and Tillotts Pharma.
Expert Insight
GI & Hepatology News invited Taku Kobayashi, MD, PhD, director of the Center for Advanced IBD Research and Treatment and co-director of the Department of Gastroenterology at Kitasato University Kitasato Institute Hospital, Tokyo, Japan, to weigh in on the study findings.
What makes this study significant?

Dr. Kobayashi: This study is important because the long-term cancer risk associated with isolated ulcerative proctitis has remained uncertain. Although previous studies suggested that CRC risk in UC is strongly associated with disease extent and appears relatively low in proctitis, most available data come from older cohorts with relatively limited numbers of patients with isolated proctitis.
This study therefore provides important contemporary evidence using a very large nationwide population-based cohort with long-term follow-up. The finding that patients with isolated ulcerative proctitis did not have an increased incidence of rectal cancer compared with matched population comparators is reassuring for both clinicians and patients.
Another important strength is that the authors performed analyses both with and without censoring follow-up at the time of proximal disease extension, which helps address an important methodological issue in UC research.
How could this study’s findings shape clinical practice?
Dr. Kobayashi: The findings generally support current European and US guideline recommendations that patients with isolated ulcerative proctitis may not require UC–specific surveillance colonoscopy programs and can instead follow standard population-based CRC screening strategies.
This is clinically important because it may help reduce unnecessary colonoscopy procedures, health care burden, and costs, while also decreasing the physical and psychological burden on patients. It may also simplify long-term management for physicians caring for patients with limited disease extent.
At the same time, surveillance decisions should still be individualized. Additional risk factors such as persistent inflammatory activity, primary sclerosing cholangitis, family history of CRC, and proximal disease extension during follow-up remain important considerations.
Where are the knowledge gaps, and what still needs investigation?
Dr. Kobayashi: One important unresolved issue is how CRC risk evolves after proximal disease extension. Approximately 40% of patients in this cohort eventually developed more extensive colitis during follow-up. Although analyses with and without censoring at extension yielded similar results, it remains uncertain whether CRC risk may increase later in patients who subsequently develop left-sided or extensive colitis.
This is important because proximal extension may occur many years after the initial diagnosis of proctitis. Therefore, the biologically relevant duration of more extensive colitis may be substantially shorter than the total study follow-up period. Since colitis-associated carcinogenesis is thought to depend on cumulative inflammatory burden over time, follow-up after extension may still be insufficient to fully evaluate long-term cancer risk associated with extended disease.
Future studies should therefore examine whether surveillance strategies should be reassessed from the time of proximal extension rather than solely from the initial diagnosis of ulcerative proctitis.
Is there anything else you'd like to say about this work?
Dr. Kobayashi: This study is a very good example of how large national registry data can answer clinically relevant questions that are difficult to address in randomized trials because cancer outcomes are fortunately uncommon and require prolonged follow-up.
I also think the study highlights the importance of individualized risk stratification in IBD surveillance rather than applying a uniform strategy to all patients with UC.
Dr. Kobayashi reported serving on advisory boards, consulting for, speaking on behalf of, and/or receiving research funding from several pharmaceutical companies.