Treatment with upadacitinib was associated with clinical response and radiologic improvement in patients with active perianal Crohn’s disease, according to a multicenter retrospective study published in Clinical Gastroenterology and Hepatology.
The study included 125 patients treated across 10 centers in the United States and Canada and evaluated both clinical outcomes and pelvic magnetic resonance imaging (MRI) findings. According to the authors, real-world data on upadacitinib in perianal Crohn’s disease have been limited, and radiologic outcomes had not previously been reported.
Perianal Crohn’s disease affects a substantial proportion of patients with Crohn’s disease and can result in fistulas, drainage, abscesses, pain and fecal incontinence. The authors noted that available treatment options have produced remission in only a minority of patients, highlighting the need for additional therapeutic approaches.
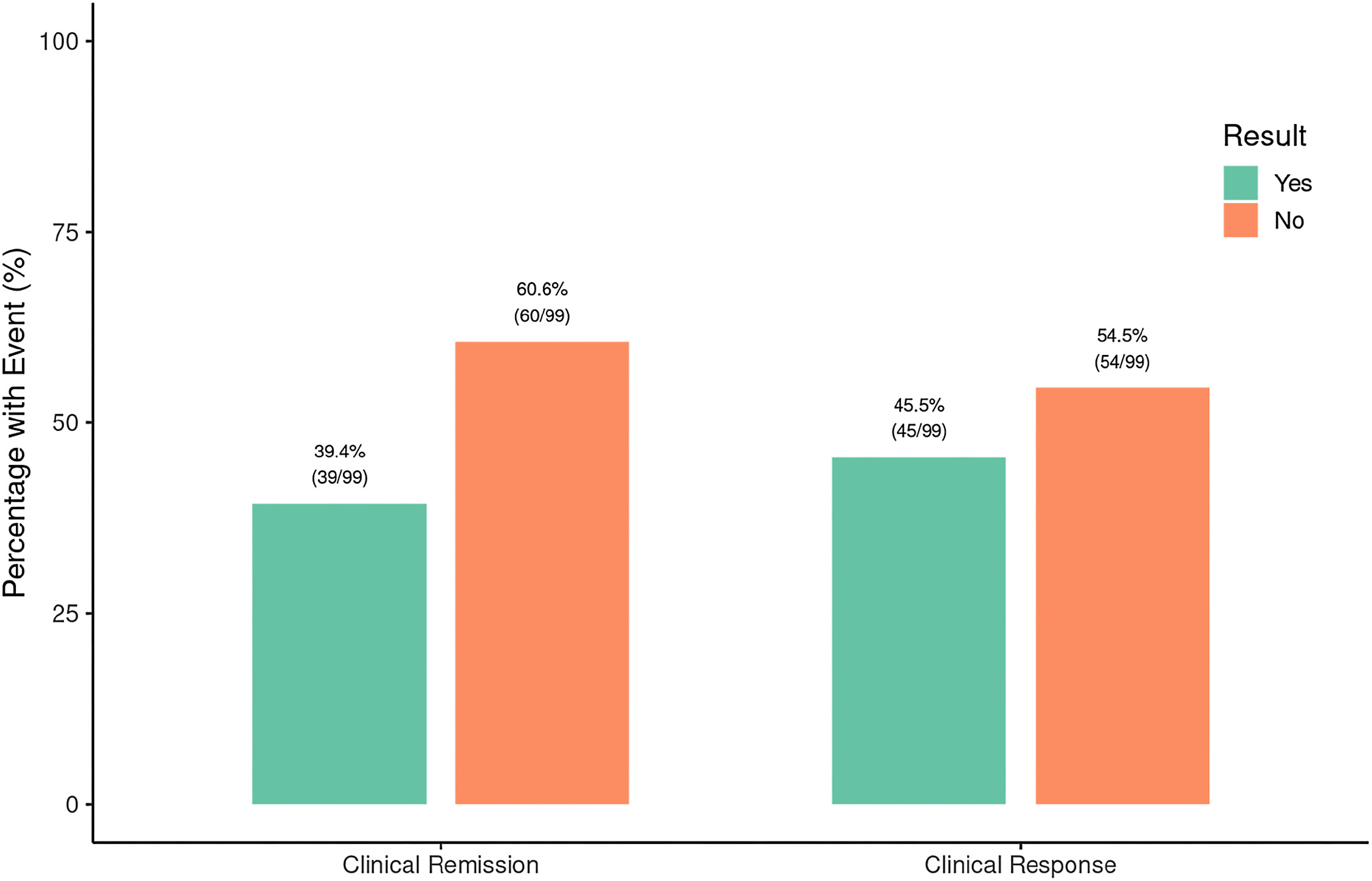
The primary outcome of the study was clinical response, defined as a reduction of at least 3 points in the perianal disease activity index. At the first follow-up visit after upadacitinib induction, 45.5% of patients achieved clinical response and 39.4% achieved clinical remission, according to the study.
Among patients who underwent follow-up pelvic MRI, 55.1% demonstrated radiologic improvement and 11.5% achieved complete healing. Overall, MRI findings improved or healed in approximately two-thirds of patients with available imaging data, according to the study.
“Treatment with upadacitinib was associated with improved fistula outcomes in patients with perianal Crohn’s disease, with greater effectiveness in those anti–tumor necrosis factor-naïve or with shorter disease duration,” the authors wrote.
The cohort included a treatment-experienced population. According to the study, nearly half of patients had complex fistulas and most had prior exposure to anti-tumor necrosis factor therapy.
Subgroup analyses identified differences in outcomes based on treatment history and disease duration. Clinical response rates were higher among patients without prior anti-tumor necrosis factor exposure than among those who had previously received anti-tumor necrosis factor therapy. Patients with a shorter duration of perianal disease also had higher response rates than those with longer-standing disease.
In multivariable analysis, prior anti-tumor necrosis factor exposure was associated with a lower likelihood of achieving clinical response.
The authors wrote that “biologic-naïve status and shorter disease duration (≤2 years) were associated with higher clinical response rates,” while prior anti-tumor necrosis factor exposure was linked to lower rates of clinical, radiologic and composite response.
The study also evaluated changes in individual perianal disease activity index domains. According to the authors, improvements were observed in measures of pain, discharge, induration and activity restriction. The authors noted that symptomatic improvement and anatomic healing may not occur at the same pace.
“This distinction underscores that [perianal disease activity index], as a composite index, may reflect symptomatic improvement without complete anatomic fistula resolution,” they wrote.

Study author Parakkal Deepak, MD, said in an interview with GI & Hepatology News that the study adds information that was not available from prior analyses of upadacitinib in perianal Crohn’s disease.
“This is, to date, the largest real-world, multicenter experience of upadacitinib specifically for perianal Crohn’s disease, and the first to report radiologic (pelvic MRI) outcomes,” Dr. Deepak said, noting that the current study evaluated both clinical response and MRI-based outcomes in routine clinical practice.
Regarding clinical implications, Dr. Deepak said upadacitinib is a “reasonable, effective option” for perianal fistulizing Crohn’s disease in real-world practice and works better the earlier it’s used. He also emphasized the role of imaging in treatment assessment.
“Practically, MRI (TOpClass) matters: clinical closure underestimates deep healing, so imaging should inform treat-to-target decisions,” he said.
The authors reported low rates of hospitalization, corticosteroid use and perianal surgery during follow-up. They wrote that these findings “underscore the clinical utility and tolerability of [upadacitinib] in this high-risk population.”
The study has several limitations. According to the authors, the retrospective observational design introduces potential bias, follow-up duration was limited, and MRI assessments were available for only a subset of patients. The study also lacked a control group, and concomitant treatments such as antibiotics and seton placement may have influenced outcomes. The authors wrote that the lack of a control group “precludes direct comparisons of effectiveness and limits causal inferences.”
They concluded that upadacitinib was “associated with meaningful clinical and radiologic benefits in patients with pCD, including those with prior biologic exposure,” while noting that prospective studies are needed to determine the durability of response over longer follow-up periods and to better define the role of upadacitinib in perianal Crohn’s disease.
Several authors reported financial relationships — including consulting, speaker, advisory board and research-support roles — with pharmaceutical and health care companies, among them AbbVie, Takeda, Pfizer, Bristol Myers Squibb, Janssen and Eli Lilly; Davenport also reported royalties from Wolters Kluwer and consulting ties to Covera Health and Roche.