A new joint consensus statement from the Rome Foundation and the International Organization for the Study of Inflammatory Bowel Disease (IOIBD), published in Gastroenterology, offers clinicians a framework for managing patients with inflammatory bowel disease (IBD) who continue to experience abdominal pain, bloating, diarrhea, constipation or mixed bowel habits despite little or no objective evidence of active inflammation — a pattern the panel termed “IBD with irritable bowel syndrome (IBS)–like symptoms.”

The recommendations address a clinical scenario the authors estimate affects roughly 20% to 30% of patients with IBD in remission, a group often subjected to repeated testing or unnecessary escalation of immunosuppressive therapy when persistent symptoms are presumed to reflect ongoing inflammation.
“This consensus study is important because it addresses a common but historically under-recognized problem in IBD care: many patients continue to experience abdominal pain, bloating, diarrhea, constipation or mixed bowel habits despite having little or no objective evidence of active inflammation. These symptoms are burdensome for patients and may lead to diagnostic uncertainty, repeated testing and sometimes unnecessary escalation of IBD-directed therapy,” said senior author Lin Chang, MD, of the David Geffen School of Medicine at UCLA, Los Angeles, who told GI & Hepatology News that the framework is meant to give clinicians a positive, mechanism-informed approach rather than a purely exclusionary one.
Using a modified RAND/UCLA Appropriateness Method, a multidisciplinary panel of 13 international experts reviewed available evidence and voted on candidate statements covering terminology, diagnosis, dietary therapies, medications and brain-gut behavioral therapies. Of 105 statements that proceeded to final scoring, 86 were rated appropriate, 16 uncertain and three inappropriate.
A central recommendation was adoption of the term “IBD with IBS-like symptoms” to describe patients with Crohn’s disease or ulcerative colitis whose symptoms are disproportionate to or incompletely explained by objective inflammation or structural bowel damage.
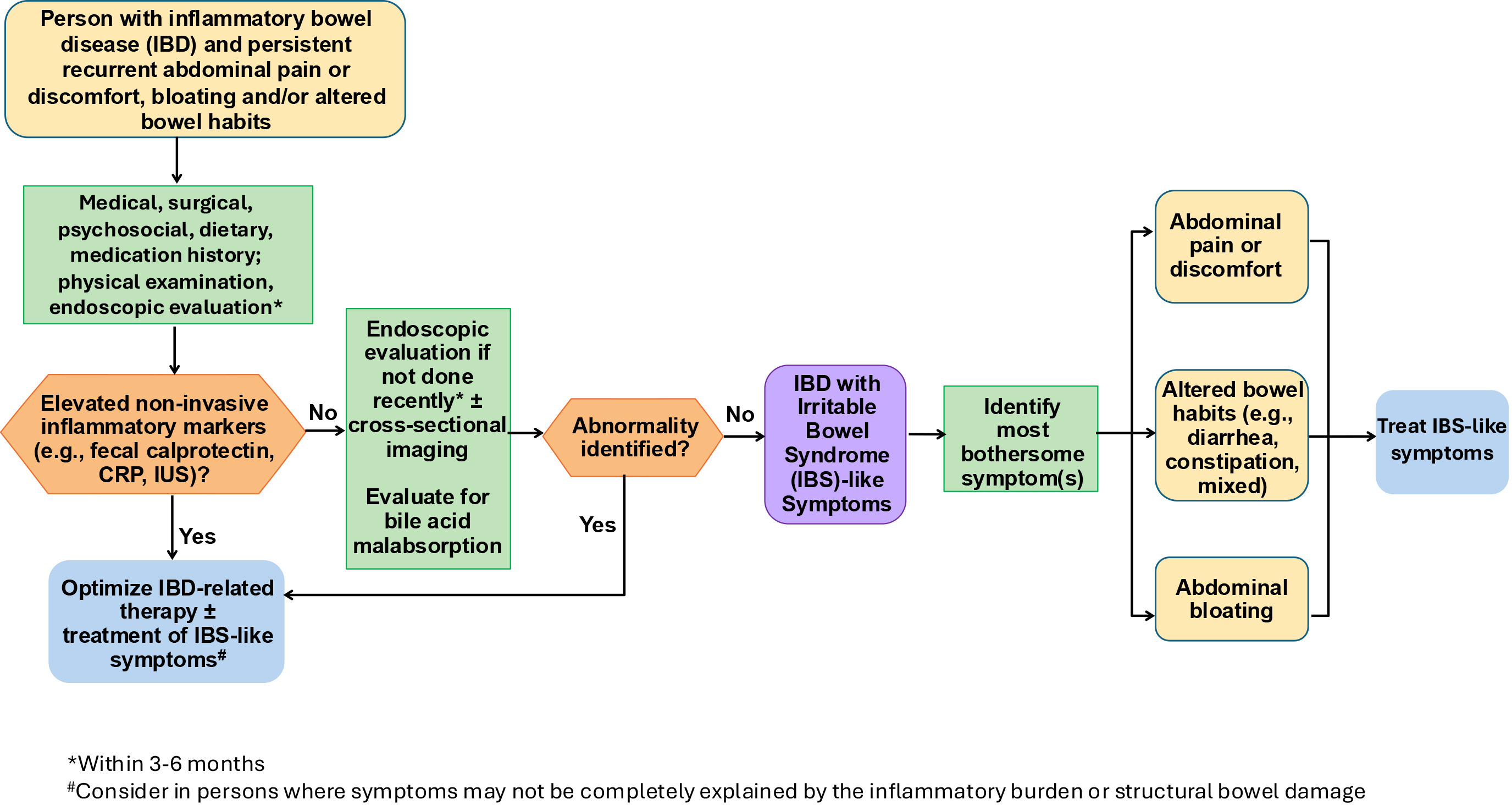
The panel proposed distinct diagnostic frameworks for clinical care and research. In routine practice, Rome clinical criteria combined with objective exclusion of active inflammation — through biomarkers, endoscopy, histology or imaging as appropriate — were considered sufficient. For research, the panel endorsed specific remission thresholds to enroll homogeneous trial populations, including a Simple Endoscopic Score for Crohn’s disease below 4, a Mayo endoscopic subscore of 0 or 1 in ulcerative colitis, and fecal calprotectin under 150 μg/g.
“The key takeaway for clinicians is that persistent gastrointestinal symptoms in a patient with IBD should not automatically be assumed to reflect active inflammatory disease,” Dr. Chang said.
For treatment, the panel endorsed psyllium supplementation in patients without clinically relevant strictures and a short-term low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet. Targeted medications were considered appropriate when matched to the predominant symptom: antidiarrheals or laxatives for bowel symptoms, with 5-HT3 antagonists in diarrhea-predominant patients and secretagogues or 5-HT4 agonists in those with constipation, provided no stricture is present. Tricyclic antidepressants received the panel’s strongest support among neuromodulators; selective serotonin reuptake inhibitors and serotonin and norepinephrine reuptake inhibitors may also be appropriate depending on stool pattern and comorbid mood or anxiety symptoms. Antispasmodics and peppermint oil were also rated appropriate.
Brain-gut behavioral therapies, including gastrointestinal-focused cognitive behavioral therapy and gut-directed hypnotherapy, received the panel’s strongest endorsement, with unanimous appropriate ratings. The authors argued these approaches should be integrated earlier in management rather than reserved as a last-line option.
“These recommendations provide a practical framework for patient care by emphasizing a positive, mechanism-informed approach rather than a purely exclusionary one,” Dr. Chang said. “Earlier recognition of this phenotype may improve quality of life, reduce unnecessary treatment escalation and help patients receive therapies that are better matched to the mechanisms driving their symptoms.”
The authors acknowledged several limitations, including heterogeneity in remission definitions across the existing literature, relatively few large randomized controlled trials specifically in patients with IBD and IBS-like symptoms, and limited mechanistic phenotyping. Many recommendations therefore relied partly on expert consensus and extrapolation from the IBS literature. The panel was also predominantly based in North America, which the authors said may limit generalizability to other regions. Patients were not included in the formal consensus process, though four individuals with IBD reviewed the near-final manuscript.
Dr. Chang and other panel members reported consulting, speaker or research relationships with pharmaceutical and digital health companies. Full disclosures are available with the published paper. The Rome Foundation provided panelist honoraria.