A new time-based prognostic model for primary sclerosing cholangitis (PSC) accurately predicted long-term risk for hepatobiliary cancer, liver transplantation, and liver-related death, and performed better than several commonly used scoring systems, according to an international validation study.
The model, known as the Helsinki PSC Score (HelPSCore), was developed from a prospective Finnish cohort of 1,016 patients with PSC and externally validated in 467 patients from Sweden and the Netherlands. Reporting in Clinical Gastroenterology and Hepatology, the investigators found area-under-the-curve values of 0.82 in the derivation cohort and 0.83 in the validation cohort for predicting the composite endpoint over as long as 25 years of follow-up.

“The HelPSCore tool assists in pinpointing high-risk patients who could benefit from enhanced monitoring and therapeutic interventions,” corresponding author Martti Färkkilä, MD, professor of gastroenterology at Helsinki University, Finland, told GI & Hepatology News. “This scoring system provides a straightforward approach for routine clinical follow-up of PSC patients and may also serve as a surrogate marker of treatment response in clinical trials.”
No disease-modifying therapy has been established for PSC, Dr. Färkkilä said, and existing prognostic models, including the Mayo Risk Score, Amsterdam-Oxford model (AOM), UK-PSC risk score, and model for end-stage liver disease (MELD), are based mainly on data collected around the time of diagnosis rather than changes in laboratory results over time. To address that limitation, he and his coauthors developed HelPSCore as a dynamic tool that uses current laboratory and imaging data rather than baseline values alone. The score incorporates disease distribution on cholangiography, specifically whether disease is confined to the intrahepatic ducts or involves both intrahepatic and extrahepatic ducts, along with levels of aspartate aminotransferase, alkaline phosphatase, bilirubin, and albumin. Higher scores indicate greater long-term risk for hepatobiliary malignancy, liver transplantation, or liver-related death.
The derivation cohort included 1,016 patients from the Helsinki University Hospital PSC registry who were diagnosed between 1990 and 2022. Patients with less than 12 months of follow-up or who reached the composite endpoint within 12 months of diagnosis were excluded. The validation cohort included 415 patients from 10 Swedish hospitals and 52 patients from the Amsterdam University Medical Center.
Investigators calculated time-weighted average values for laboratory measurements collected during follow-up. Patients in the derivation cohort underwent an average of five laboratory assessments, with a mean of 272 days between tests. The primary endpoint was the first occurrence of hepatobiliary malignancy, liver transplantation, or liver-related death.
According to the investigators, the strongest predictors of adverse outcomes were elevated levels of aspartate aminotransferase, alkaline phosphatase, and bilirubin, lower albumin levels, and disease involving both the intrahepatic and extrahepatic bile ducts. Patients with both intrahepatic and extrahepatic disease had a 3.69-fold higher risk for the composite endpoint than those with intrahepatic disease alone.
The investigators found that about 30% of patients with disease limited to the intrahepatic bile ducts progressed to disease involving both the intrahepatic and extrahepatic bile ducts during follow-up. Patients with combined disease involvement had a substantially higher cumulative incidence of adverse outcomes than those with intrahepatic disease alone.
Among laboratory variables, time-weighted aspartate aminotransferase values showed particularly strong predictive performance, with an area under the curve of 0.88 in patients with intrahepatic disease, according to the paper. Albumin and bilirubin also demonstrated strong prognostic value across disease subtypes, investigators reported.
Overall, the model achieved a positive classification rate of 91%, a negative classification rate of 56%, and an overall correct classification rate of 86%.
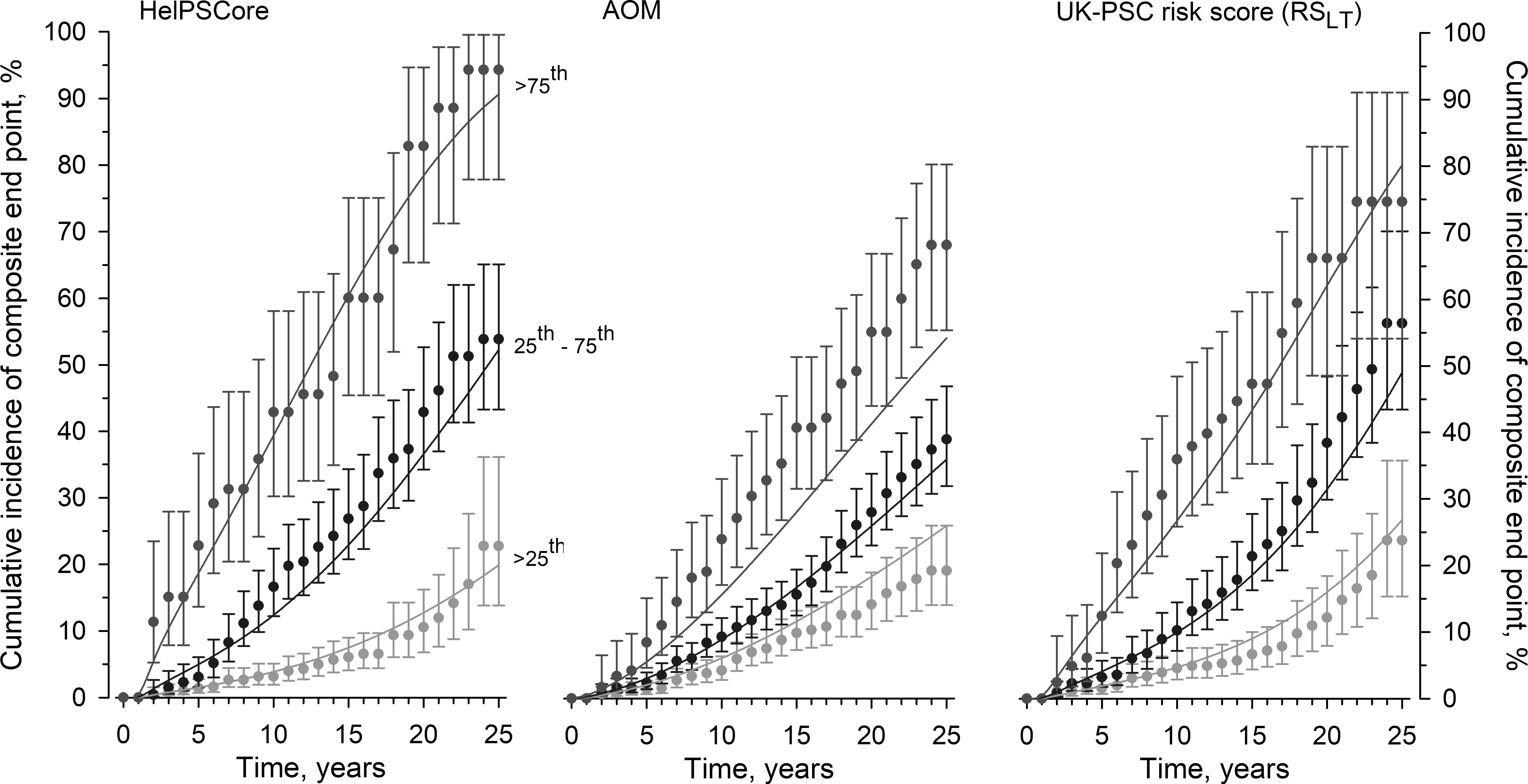
The study also compared HelPSCore with existing prognostic models. Over both short- and long-term follow-up, HelPSCore consistently demonstrated higher Harrell’s C statistics than the AOM, UK-PSC risk score, Mayo model, and MELD score.
“This is the first time dependent dynamic prognostic score for PSC overperforming the earlier published scores,” Dr. Färkkilä said. “Assessing disease trajectory and overall prognosis in patients with PSC remains challenging because of the marked heterogeneity in clinical course. HelPSCore may improve risk stratification and prediction of disease outcomes, thereby enabling more individualized surveillance and management strategies.”
The investigators reported that the 25-year cumulative risk for the composite endpoint exceeded 95% among patients with a HelPSCore of 5 or higher, but remained below 5% for patients with scores of 1 or less.
Rates of major clinical events were similar between derivation and validation cohorts. Liver transplantation occurred in 96 patients in the derivation cohort and 78 patients in the validation cohort, corresponding to incidences of 8.3 and 9.9 per 1,000 patient-years, respectively. Cholangiocarcinoma developed in 31 and 17 patients, respectively.
The authors acknowledged limitations of the analysis. Assessing disease extent required cholangiography, ideally high-quality magnetic resonance cholangiopancreatography, and many patients in the Dutch validation cohort were excluded because disease distribution data were missing. The model also did not account for possible confounding factors such as medications, endoscopic procedures, or other medical conditions.
The study was funded by the Finnish Cancer Foundation and the State Funding for University-level Health Research. The authors reported no conflicts of interest.