Early detection of pancreatic cancer through targeted screening of high-risk patients may improve survival by identifying disease at a surgically curable stage, according to Shifa Umar, MD.
During a wide-ranging lecture at Digestive Disease Week® (DDW) 2026, Dr. Umar, assistant professor of medicine in the section of gastroenterology and hepatology at Baylor College of Medicine, Houston, noted that pancreatic ductal adenocarcinoma is now the third leading cause of cancer-related death in the US, with a five-year survival of 37% for localized disease that falls to 3% in patients with distant metastases. Because surgery provides the best chance for long-term survival, screening efforts are increasingly focused on finding tumors before symptoms appear.
The US Preventive Services Task Force does not recommend screening asymptomatic adults at average risk, citing the disease’s low incidence, uncertain accuracy of available screening tools, and poor overall prognosis. However, Dr. Umar, who also directs the Pancreas Center of Excellence at the Michael DeBakey VA Medical Center, emphasized that screening recommendations vary significantly for patients with a family history or genetic risk factors.
About 5% to 10% of pancreatic cancers are associated with familial risk, she said. Familial pancreatic cancer is defined as a kindred with pancreatic cancer occurring in two or more first-degree relatives. Risk increases as the number of affected first-degree relatives rises.
Several germline mutations and inherited syndromes are also associated with elevated risk. According to Dr. Umar, the highest-risk groups include patients with STK11 mutations associated with Peutz-Jeghers syndrome, PRSS1 mutations associated with hereditary pancreatitis, and CDKN2A mutations associated with familial atypical multiple mole melanoma syndrome. Moderate-risk groups include patients with BRCA-associated syndromes, Lynch syndrome, Li-Fraumeni syndrome, and ATM mutations.
Current National Comprehensive Cancer Network recommendations call for germline genetic testing in all patients diagnosed with pancreatic cancer and in all patients with a first-degree relative with pancreatic cancer. Screening should be performed within high-volume pancreatic cancer centers, Dr. Umar said.
She highlighted recent guideline changes expanding eligibility for surveillance. As of 2025, patients with ATM and BRCA2 mutations are recommended for pancreatic cancer screening regardless of family history.
Chronic pancreatitis remains a recognized risk factor, with meta-analyses showing up to a 16-fold increased risk of pancreatic cancer. However, Dr. Umar noted that only a small proportion of patients with chronic pancreatitis ultimately develop malignancy, limiting its utility as a standalone indication for screening.
Modifiable risk factors discussed during the lecture included tobacco use, heavy alcohol consumption, and obesity. Dr. Umar noted that every five-unit increase in body mass index is associated with a 10% increase in pancreatic cancer mortality risk. Although these factors do not independently justify screening, they remain important targets for risk reduction counseling.
Among emerging screening approaches, Dr. Umar identified new-onset diabetes as one of the most promising opportunities for earlier detection. The Enriching New-Onset Diabetes for Pancreatic Cancer (ENDPAC) score, developed at Mayo Clinic in 2018, incorporates age at diabetes onset, changes in blood glucose, and weight loss to stratify patients. Patients with scores greater than three are considered high risk and can be suggested candidates for diagnostic imaging.
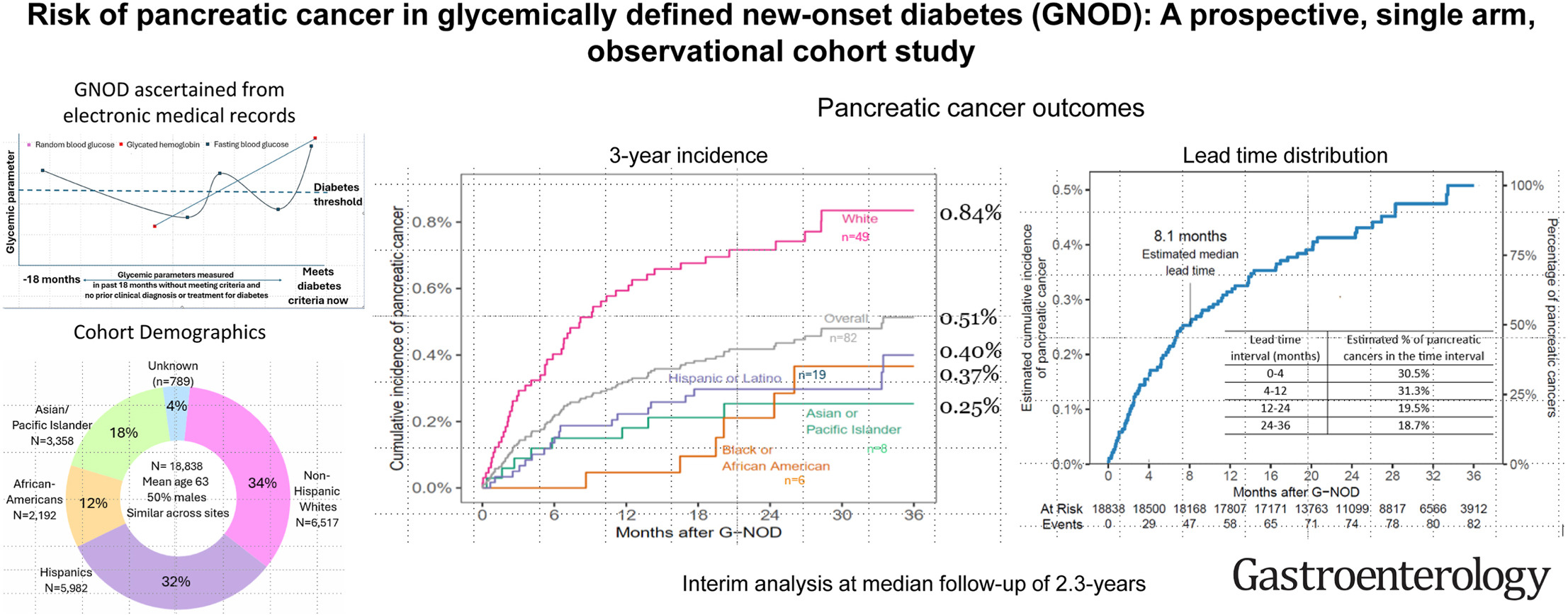
She also highlighted a prospective study published in Gastroenterology by investigators at MD Anderson Cancer Center that used real-time electronic medical record surveillance to follow patients with glycemic new-onset diabetes for up to two years. Patients with glycemic new-onset diabetes had a fivefold increased risk of pancreatic cancer, with an estimated lead time to diagnosis of eight to 12 months. The highest risk was observed among White patients.
Dr. Umar said her clinical approach begins with identifying patients with glycemic new-onset diabetes, followed by risk stratification using the ENDPAC score. High-risk patients can be considered for magnetic resonance imaging (MRI) or endoscopic ultrasound (EUS). Low-risk patients continue routine follow-up.
For imaging surveillance, Dr. Umar emphasized that MRI and EUS should be viewed as complementary rather than competing modalities. She cited a study which showed that computed tomography (CT) and EUS together missed cystic lesions later identified on MRI, while CT and MRI missed lesions subsequently detected by EUS.
EUS may be preferred in patients with Lynch syndrome or Peutz-Jeghers syndrome who already require endoscopic evaluation, she said, as well as in patients with contraindications to MRI. MRI may be preferred in patients seeking less invasive screening.
Surgical referral is recommended for patients with high-risk pancreatic cysts, or biopsy-confirmed high-grade dysplasia or malignancy, ideally after multidisciplinary review.
Dr. Umar also referenced data from pancreatic cancer surveillance programs demonstrating improved outcomes among screened patients. Median survival reached five years in screened cohorts compared with 1.4 years in control groups, with higher rates of resectability and earlier-stage diagnosis.

Looking ahead, Dr. Umar highlighted artificial intelligence and radiomics as emerging tools that may detect imaging abnormalities invisible to radiologists. Blood-, saliva-, and stool-based biomarkers are also under investigation for earlier disease detection.
“Pancreatic cancer screening is not a one-size-fits-all approach,” Dr. Umar said. “These patients need to be risk stratified and then need appropriate follow-up based on underlying genetic mutation, familial risk, and other variables.”
Dr. Umar reported having no disclosures.
DDW is AGA’s annual meeting, jointly sponsored by AGA, AASLD, ASGE, and SSAT. Learn more at ddw.org.