Patients with ulcerative colitis (UC) who stopped thiopurines shortly after starting anti-tumor necrosis factor (TNF) therapy had a modestly higher risk of adverse clinical outcomes than those who continued combination treatment, according to a nationwide Korean cohort study published in Clinical Gastroenterology and Hepatology. Stopping thiopurines did not significantly worsen outcomes in patients with Crohn's disease (CD).
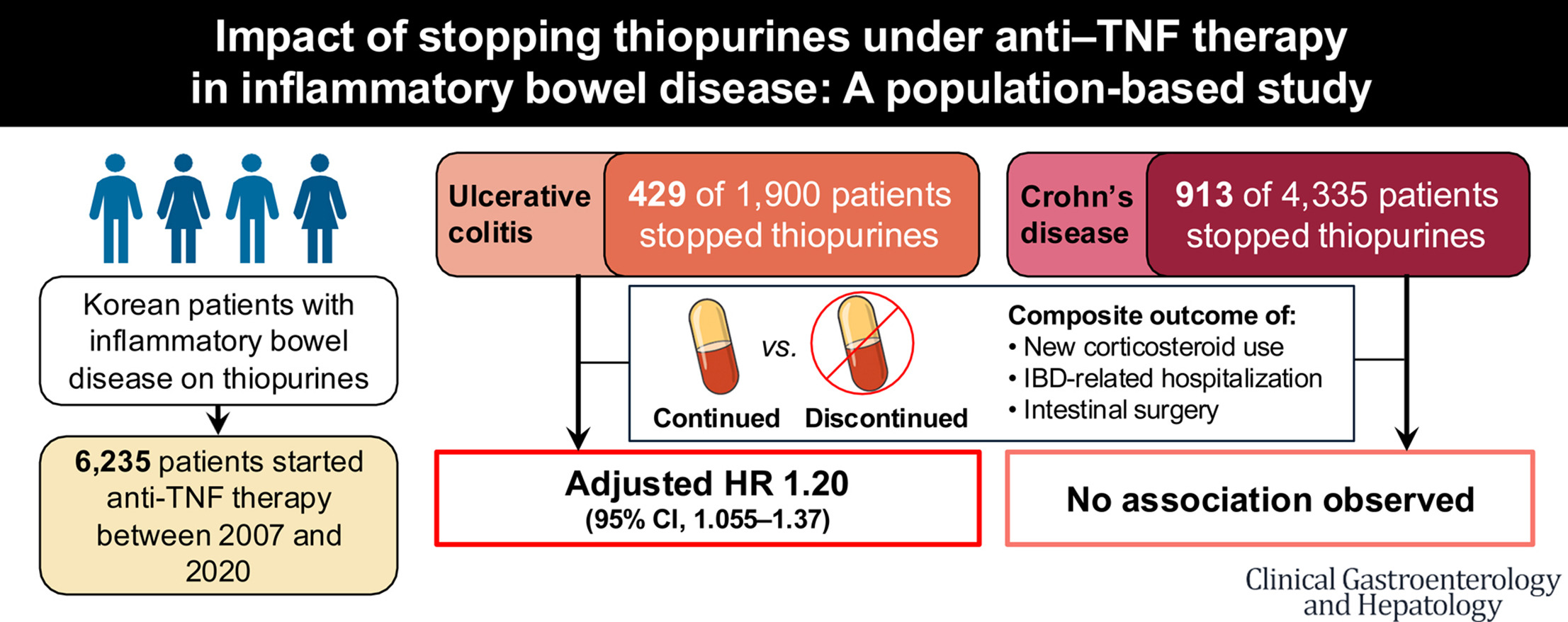
The retrospective population-based study analyzed Korean National Health Insurance claims data from 6,235 patients with inflammatory bowel disease (IBD) who initiated anti-TNF therapy between 2007 and 2020 while receiving thiopurines.
“Discontinuing thiopurines after initiating anti-TNF therapy in patients with UC may modestly increase the risk of adverse outcomes,” wrote the investigators, led by senior author Byong Duk Ye, MD, PhD, of the Department of Internal Medicine at Chung-Ang University College of Medicine in Seoul, Korea. “Thus, caution is recommended when considering thiopurine withdrawal in patients with UC.”
The investigators classified patients according to whether they continued or discontinued thiopurines within 90 days of starting anti-TNF treatment. The primary endpoint was a composite of new corticosteroid use, IBD-related hospitalization, or intestinal surgery occurring at least 90 days after anti-TNF initiation.
Among the cohort, 1,900 patients had UC and 4,335 had CD. About 22% of patients in each disease group discontinued thiopurines within 90 days. Median follow-up was four years.
In UC, discontinuation was associated with a 20% higher risk of the composite outcome and an 18% higher risk of new corticosteroid use after adjustment for confounding variables. The composite outcome occurred at a rate of 53 events per 100 person-years in the discontinuation group compared with 42 events per 100 person-years among patients who continued thiopurines. However, stopping thiopurines was not independently linked to a higher risk of hospitalization or surgery in patients with UC.
For CD, no significant differences emerged between continuation and discontinuation groups for the composite endpoint, corticosteroid use, hospitalization, or surgery after multivariable adjustment. Composite outcome rates were 37 vs. 33 events per 100 person-years in the discontinuation and continuation groups, respectively.
Sensitivity analyses using a 180-day landmark definition for discontinuation produced consistent results.
Subgroup analyses suggested that patients with UC receiving infliximab were particularly vulnerable after thiopurine withdrawal, with a 24% higher risk of adverse outcomes after discontinuation; no significant increase was seen with adalimumab.
Longer-term treatment patterns offered a more nuanced picture. Patients who were able to stop thiopurines for at least one year did not have significantly higher risks of poor outcomes in either UC or CD. In contrast, patients who stopped thiopurines but later restarted them had much higher risks of adverse outcomes — especially in UC, where restarting treatment was linked to an 80% increase in the odds of adverse events.
Cancer incidence did not significantly differ between continuation and discontinuation groups during follow-up, although the number of malignancies was low and the study was not powered for long-term cancer outcomes.
The authors acknowledged limitations including the study's retrospective design and the lack of detailed clinical data such as endoscopic findings, disease activity scores, anti-drug antibody levels, and anti-TNF drug concentrations. The claims database also could not show why thiopurines were stopped or whether patients took their medications as prescribed.
The study was supported by grants from the National Research Foundation of Korea and Chung-Ang University Research Grants. Dr. Ye reported consulting fees, speaker fees, or research support from AbbVie, Pfizer, Takeda, Celltrion, Samsung Bioepis, and Johnson & Johnson Korea. The remaining authors reported no relevant conflicts of interest.